(EWR comment) A woman returning to NZ from Ireland politely and respectfully declines to be PCR tested. That appears to incur not only a longer stay but an interesting train of events. It is clearly an option on the official forms to decline. Thereafter, listen to her describe the bizarre events that unfolded, including a surveillance cam plus a member of the military 24/7 right outside her hotel door. At the close of the tale, as she is leaving, escorted with her bags by another military member, he likens her stay to ‘solitary confinement’. (Remember the Canadian post recently when a person only managed to escape from quarantine by paying money?)
The German Philosopher Johann Von Goethe, once said, there are none more hopelessly enslaved, than those who falsely believe they are free.
But few who hear the words realize that they are the ones to whom Goethe was referring for the reality is that every person in the civilized world is enslaved from childhood. They are enslaved in a prison without walls or bars and so few ever even realize it but all are enslaved none the less. And what the people of the world are enslaved to, is a system of perpetual self generating debt that is created for them wholly by design by private international banking interests, and the people are taught from an early age to just accept this debt, because this is ‘just the way things are’ but the real reality is that it is not just the way things are, but more the way things have been designed and all one has to do is glance around them at the state of the world today to realise that though this is the way things current are, it is most definitely not the way things should be.
The most powerful and useful tool a person can ever gain in their life is knowledge for with knowledge comes wisdom and a deeper understanding and real truth can be exhilarating because real truth will set you free.
Now whether you believe in the Illuminati or not, whether you will take the time to listen to so called conspiracy theories or not, there are some things that should be clearly understood by all and these are not conspiracy theories by any stretch of the imagination, they are well documented, quite traceable and very provable facts and these facts are as follows.
Join Claire Deeks from Voices For Freedom when she catches up with Ivor Cummins talking about the global response to Covid19.
Ivor Cummins BE(Chem) CEng MIEI PMP is a Biochemical Engineer who has spent over 25 years in corporate technical leadership and management positions. His career specialty has been leading large worldwide teams in complex problem-solving activity. Since 2012 Ivor has been intensively researching the root causes of modern chronic disease. A particular focus has been on cardiovascular disease, diabetes and obesity. Since March 2020, Ivor has dedicated his analytical and biochemical expertise to deep and revealing analysis of the Covid19 pandemic situation.
In this podcast Ivor and Claire discuss the following:
[02:52] Ivor’s background in low-carb and how this investigation of the corruption in the food industry.
[06:58] How his corporate problem-solving background informs his views on the COVID-19 response.
[08:31] The corruption of the WHO and the changing definition of “pandemic” and the real severity of the virus.
[10:19] The New Zealand situation – why its been a failed experiment, a look at QALYs and the average age of death versus average age of COVID-19 death.
[14:50] Lockdowns and all the science and real word experience and now published papers that show they don’t work.
And, from this, Israel’s “health” authorities conclude that the solution (final?) is more “vaccination.”
“Our free press” continues to (a) black out the fact that most of those who have fallen ill, allegedly with COVID-19, were “vaccinated,” while (b) spreading the Big Lie, enabled by the CDC’s cooked numbers, that the opposite is true.
That’s not just propaganda, but propaganda at its most poisonous, as it’s laying the psychic groundwork for what’s coming next (if They should have Their way): scapegoating of the “unvaccinated,” followed by their forcible injection and/or mass arrest.
In light of what’s at stake, we need strong and unrelenting protest, not of any state or federal “health” agencies, but of the media outlets blacking out the truth with that Big Lie. Their offices and networks should be hit with (peaceful) protests that they can’t ignore.
From David Diamond:
A vaccinated kid infects 83 mostly vaccinated kids at a party. The virus is traced to his vaccinated uncle and then to another vaccinated carrier.
If this is 95% efficacy, I hate to see what would happen if the vax didn’t work.
By the way, the conclusion of the Israeli health authorities was more vaccination.
Kiwis are outraged at this announcement. Increasingly ‘they’ (NZ govt) are referring to ‘when’ folk are ‘vaccinated’ and not ‘if they choose to be’. From a govt that said originally there would be no mandatory, this is not-so-subtle coercion at best.
At the link here is a wide coverage of this new development announced by NZ’s Chris Hipkins, taking in NZ TV interviews & announcements plus the wider issues of numbers in the US (deaths & adverse events) including the expertise of eminent Cardiologist Dr Peter McCullough. (Video by Coronavirus Plushie channel).
Did you catch the official disinformation today? [From Dr Michael Baker]. We wonder if The AM Show will find their integrity and publish a correction? How completely clueless are these people? Or was this more than clueless? How can a top scientific “expert” be so ill-informed? Stay informed, incredible people! www.voicesforfreedom.co.nz/join-us
Distraught people who trusted the system. As I’ve noticed myself listening to the many videos & reports by innocent folk who lined up trustingly to take the shot that would protect them so they could travel and return to normal, let down & betrayed by the system. Folks they are not promising you’ll be protected at all. The best they can do is mitigate symptoms. And the vaxxed are getting the CV anyway. Proceed at your own risk. At least read the evidence. The dismayed folk called us conspiracy theorists and even scoffed and mocked us. Now they pay, sometimes with their very lives. Please do listen to the warnings. And read. Read the very real evidence that we now have to look at. Ask yourself why do they not want you seeing VAERS?
Comments by Brian Shilhavy Editor, Health Impact News
Over 6 months into the mass vaccination campaign with the experimental, non-FDA approved COVID-19 shots, where about half of the U.S. population now has received at least one of these injections, tens of thousands of victims are beginning to speak out, regretting their choices, and begging for help.
The medical community by and large has turned their backs on them, which is really what they have done for the past 40+ years with ALL vaccine injured people, most of whom have been children prior to the COVID-19 shots.
So while those speaking out in the past have been primarily parents of vaccine-damaged children that the corporate media and medical system have summarily dismissed as “crazy,” now those speaking out are primarily adults who have had their lives ruined by these injections. Pro-vaccine adults, obviously, since they chose to receive one of these shots, that many dissenting medical doctors and scientists are now calling “bioweapon” shots.
At least they still have a voice to speak out, as thousands of others are now dead following the shots, according to CDC statistics.
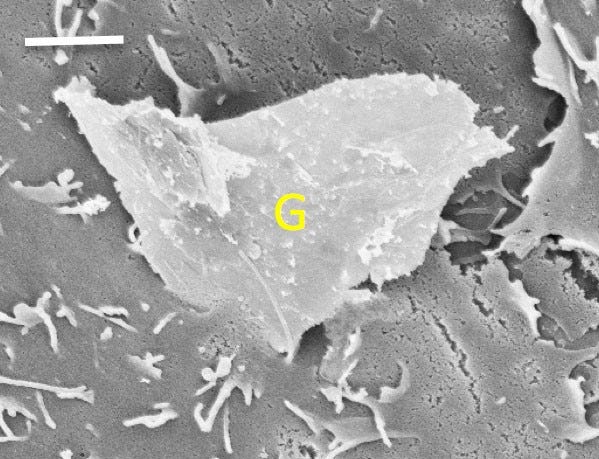
“The toxicity of graphene oxide is reason enough to stop the global vaccination program.”
Amen to that; and, as we push for an immediate end to those injections, because of their high graphene oxide content, we also need to spread the word that those paper masks are also treated with graphene—a fact that made some few headlines in April, when Health Canada banned the wearing of such masks in schools and daycare facilities throughout Quebec. Here are two detailed pieces on the dangers of graphene inhalation: https://www.aier.org/article/the-dangers-of-masks/ https://newatlas.com/graphene-bad-for-environment-toxic-for-humans/31851/
So there’s graphene in those “vaccines” that many millions have been led to think will save them from COVID-19, and there’s also graphene on the masks that many millions have been wearing for months and months, thinking that such self-suffocation will protect them from COVID-19; and there’s also graphene on the PCR swabs that have been shoved up many millions of tense noses, ostensibly to test for COVID-19. Check out this (fittingly) breathless item from Graphene-info.com: https://www.graphene-info.com/new-graphene-biosensor-can-detect-sars-cov-2-under-minute
Thus COVID-19 World is all about graphene—a toxin that itself causes the symptoms of both COVID-19 and the “vaccination” injuries that “our free press” is laboring to conceal.
I suggest that we think long (but not too long) and hard about all this—and that we do so while each sipping pine needle tea, which, as Celia Farber reminds us here, is a widely available antidote to what They’re (literally) banking on injecting into every single one of us.
KHUSHAB, PUNJAB — A police superintendent is dead in what may be the fastest death we’ve covered on this blog.
Mr. Malik Imtiaz Mahmood was the Superintendent of Police for the city of Khushab. He received his experimental injection against COVID-19 on or around June 13, according to the World Doctors Alliance. The organization shared a photo of Mr. Mahmood receiving the injection.
Read more below (video included as the superintendent collapses):
“Let’s face it – there is no way our small blog can report on every event related to COVID dystopia. We didn’t even have time in this article to write about California McDonald’s restaurants now offering vaccinations. Some locations are offering a free Big Mac right after you get the experimental “McVaccine” in their super-clean, sanitary dining rooms. Of course the Centers for Disease Control admitted long ago that nearly 80% of COVID-19 hospitalizations are overweight and obese people.
Regardless, in our efforts to keep you up-to-date on all the latest happenings, we do one of these summary articles every month. Here are seven stories that were suppressed and/or censored by mainstream media and big tech in June.
This week’s number of total adverse events for all age groups following COVID vaccines surpassed 400,000, according to data released today by the Centers for Disease Control and Prevention (CDC). The data comes directly from reports submitted to the Vaccine Adverse Event Reporting System (VAERS).
VAERS is the primary government-funded system for reporting adverse vaccine reactions in the U.S. Reports submitted to VAERS require further investigation before a causal relationship can be confirmed.
Every Friday, VAERS makes public all vaccine injury reports received as of a specified date, usually about a week prior to the release date.
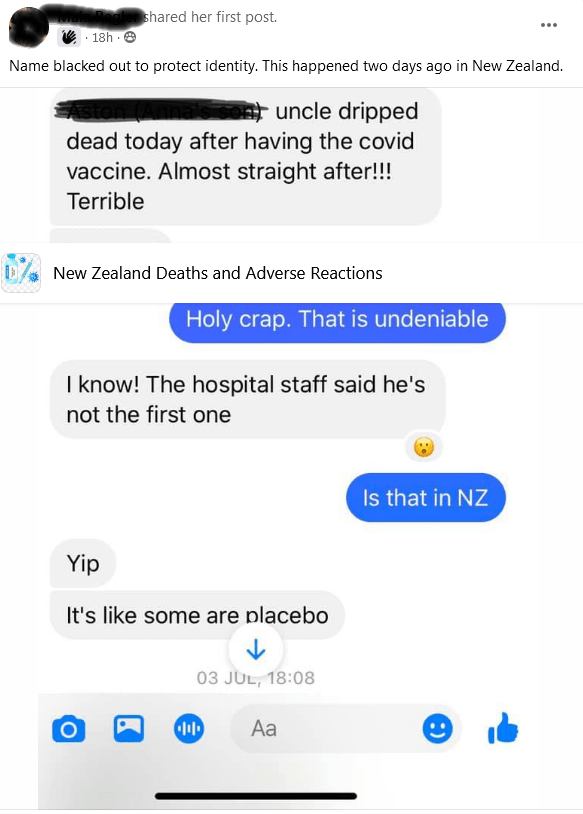
Below is a fb screenshot of the testimony of the death of a relative (names removed):
A New Zealander from the South Island has had a serious adverse reaction to the experimental injection. I am summarizing their statement from fb here so as not to identify the person, but also to illustrate to you what is happening. To alert you to possible adverse events that our NZ Doctors are not allowed to tell us. (The FDA lists a very different group of possible outcomes to those listed on NZ’s health website. Info below with links).
The jab in this instance required an ambulance to be called the following day as the patient was experiencing dizziness, shortness of breath, nausea, diarrhea, fever, confusion, loss of appetite, stomach pain, weakness & shaking and fatigue.
A high temperature, nearly 40.
Drips and pain medication were administered in hospital. Heart rate erratic. Five hours to come reasonably right and still not fully okay.
The patient’s been told by the health authority that if they don’t get the second shot they will get hit badly if they get CV and deny that the adverse reaction had anything to do with the VX.
IMPORTANT INFO: About the covid-19 jab, consider the following info not provided by the NZ govt:
KNOWN POSSIBLE SIDE EFFECTS FROM THE COVID-19 EXPERIMENTAL mRNA INJECTION
This is a draft list compiled by the FDA – the Food and Drug Administration in the US (link below):
You aren’t necessarily going to get all of those or even any of them if you have the vaccine. But those are the possible side effects that the FDA has listed. They’re all unpleasant, most of them very serious and you can’t get more serious than death. Below are the deaths & injuries reported to the official government data bases that occurred after taking the covid-19 injection. Remember only 1% on average are reporting.
CURRENT DEATH & INJURY STATS REPORTED: (links to reporting sites below)
USA: DEATHS – 4,863 INJURIES: 262,521 (to June 24 )
UK: 1,295 DEATHS – INJURIES 922,596 (to June 10th)
EUROPE: 13,867 – INJURIES 1,354,336 (to June 5th)
AUSTRALIA – 210 DEATHS – 22031 INJURIES (to 27 May)
As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection.
U.S. soldiers administer COVD-19 vaccines at Fort Hood, Texas, Feb. 20, 2021. (U.S. Army photo/Staff Sgt. Daniel Herman)
The Army has directed commands to prepare to administer mandatory COVID-19 vaccines as early as Sept. 1, pending full Food and Drug Administration licensure, Army Times has learned.
The directive came from an execute order sent to the force by Department of the Army Headquarters.
Army Times obtained a portion of a recent update to HQDA EXORD 225-21, COVID-19 Steady State Operations.
“Commanders will continue COVID-19 vaccination operations and prepare for a directive to mandate COVID-19 vaccination for service members [on or around] 01 September 2021, pending full FDA licensure,” the order said. “Commands will be prepared to provide a backbrief on servicemember vaccination status and way ahead for completion once the vaccine is mandated.”
EXORDS are utilized when the president directs the defense secretary to execute a military operation.
“As a matter of policy we do not comment on leaked documents. The vaccine continues to be voluntary,” said Maj. Jackie Wren, an Army spokesperson. “If we are directed by DoD to change our posture, we are prepared to do so.”
The Pentagon has not put out any guidance to the services to prepare for a mandatory vaccine roll-out in September, a defense official separately told Army Times.
It was not immediately clear whether the vaccines would even be approved in time for a Sept. 1 mandatory rollout. And an FDA spokesperson did not have an exact timeline available.
The ”timelines for vaccine approval may vary depending on a number of factors, but as Pfizerand Moderna announced, they have initiated rolling submissions of their biologics license applications for their COVID-19 vaccines,” said Alison Hunt, an FDA spokesperson. “As a general matter, FDA cannot comment on particular applications.”
Once the companies finish collecting biologics license application data on their vaccines, the FDA will take 60 days to review the applications for full approval, in accordance with the agency’s guidelines for priority review.
The Army currently has around 70 percent of its force vaccinated against the coronavirus, according to Army Lt. Gen. Ronald Place, director of the Defense Health Agency.
However, demand for the vaccine has fallen off in recent months across the military, roughly following a similar drop in demand among the American people.
The Veterans Affairs administration is currently weighing a plan to require all VA staffers to receive the vaccine, amid growing worry worldwide about the more severe Delta variant of the virus.
The Navy also recently told sailors to expect a mandatory vaccination program despite having the highest vaccine acceptance rate thus far.
Military Times Pentagon bureau chief Meghann Myers contributed to this report.
EWR note: I have just spent at least 20 minutes trying to edit another post… everything all over the place. I note also that the fb share icon has disappeared again as it frequently does these days. (The one that numbers shares)…. Below is info I’ve gathered from a post documented on fb FYI. Consider the info available given MDs have been largely silenced from giving you any fuller picture of possible outcomes, other than ‘safe & effective’.
Here sadly is the testimony of a young father. Remember what happens to this man as you ponder: there’s little in the various rhetoric & reports to assure that they have your back. We’ve seen denial of any connection between the jab & the adverse event, and frequently, denial of (or inability to even find) treatment. Do please consider his Go Fund Me plea. Remember the Pharma corporations have complete freedom from liability for their ‘safe & effective’ jabs. EWR
Immediate reaction to the Moderna Covid vaccine
“On May 25, 2021 Freddy suffered an immediate and severe reaction to his Moderna COVID vaccination. Within the 15 minute waiting period the left side of his body was paralyzed, he went cold, and his breathing became extremely shallow. He had swelling in his feet and a rash throughout his body. Freddy was treated immediately on site by paramedics. The following night he experienced dizziness and heart palpitations, collapsed in his home and stopped breathing. Freddy’s heart went into major atrial fibrillation and he was transported back to the hospital where a loop recorder was implanted into his chest to monitor his heart. Since then he has had six seizures and/or strokes (to be determined), experiences constant uncontrollable spasms and tremors, migraines, tinnitus, fatigue, dizziness, brain fog, and overall body pain. Freddy is a self-employed roof contractor with two children, aged 10 and 14. He is unable to work or drive, and has difficulty walking. Since his injury he has been unable to receive proper medical care in his home town, and has been dismissed and ignored by various health care providers. He is in need of many exams, test, scans, bloodwork, and to find a medical team willing to treat him. This is very likely to include travel and various other expenses. Freddy is in need of support from his community and fellow humans to assist with these impending costs, and to care for his family.”
If you care to you can see his adverse reaction at the link:
While the list of crimes committed by authorities during the COVID-19 pandemic is a long one, perhaps the biggest crime of all is the purposeful suppression of safe and effective treatments, including ivermectin. This appears to have been done to protect the COVID “vaccine” program
The COVID shots were brought to market under emergency use authorization (EUA), which can only be obtained if there are no other safe and effective alternatives available
Several systematic reviews and meta-analyses of studies looked at ivermectin for the prevention and treatment of COVID-19 infection. A rapid review performed on behalf of the Front Line COVID-19 Critical Care Alliance (FLCCC) in the U.S., January 3, 2021, found the drug “probably reduces deaths by an average 83% compared to no ivermectin treatment”
According to a more recent review and meta-analysis, ivermectin, when used preventatively, reduced COVID-19 infection by an average 86%
Another recent scientific review concluded ivermectin produces large statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance
While the list of crimes committed by authorities during the COVID-19 pandemic is a long one, perhaps the biggest crime of all is the purposeful suppression of safe and effective treatments. At this point, it seems quite clear that this was done to protect the COVID jab rollout.
The COVID shots were brought to market under emergency use authorization (EUA), which can only be obtained if there are no other alternatives available. In a sane world, the COVID gene therapies would never have gotten an EUA, as there are several safe and effective treatment options available.
One treatment that stands out above the others is ivermectin, a decades-old antiparasitic drug that is on the World Health Organization’s list of essential medications.
What makes ivermectin particularly useful in COVID-19 is the fact that it works both in the initial viral phase of the illness, when antivirals are required, as well as the inflammatory stage, when the viral load drops off and anti-inflammatories become necessary. It’s been shown to significantly inhibit SARS-CoV-2 replication in vitro,1 speed up viral clearance and dramatically reduce the risk of death.
Gold Standard Review Supports Use of Ivermectin
Dr. Tess Lawrie, a medical doctor, Ph.D., researcher and director of Evidence-Based Medicine Consultancy Ltd (video above).2 in the U.K., has been trying to get the word out about ivermectin. To that end, she helped organize the British Ivermectin Recommendation Development (BIRD) panel3 and the International Ivermectin for COVID Conference,4 which was held online, April 24, 2021.
Twelve medical experts5 from around the world shared their knowledge during this conference, reviewing mechanism of action, protocols for prevention and treatment, including so-called long-hauler syndrome, research findings and real world data. All of the lectures, which were recorded via Zoom, can be viewed on Bird-Group.org.6
Lawrie has published several systematic reviews and meta-analyses of studies looking at ivermectin for the prevention and treatment of COVID-19 infection. A rapid review performed on behalf of the Front Line COVID-19 Critical Care Alliance (FLCCC) in the U.S., January 3, 2021, found the drug “probably reduces deaths by an average 83% compared to no ivermectin treatment.”7
Her February 2021 meta-analysis, which included 13 studies, found a 68% reduction in deaths. This is an underestimation of the beneficial effect, because one of the studies included used hydroxychloroquine (HCQ) in the control arm. Since HCQ is an active treatment that has also been shown to have a positive impact on outcomes, it’s not surprising that this particular study did not rate ivermectin as better than the control treatment (which was HCQ).
Two months later, March 31, 2021, Lawrie published an updated analysis that included two additional randomized controlled trials. This time, the mortality reduction was 62%. When four studies with high risk of bias were removed during a subsequent sensitivity analysis, they ended up with a 72% reduction in deaths.
(Sensitivity analyses are done to double-check and verify results. Since the sensitivity analysis rendered an even better result, it confirms the initial finding. In other words, ivermectin is unlikely to reduce mortality by anything less than 62%.)
Lawrie reviewed the February and March analyses and other meta-analyses in an interview with Dr. John Campbell, featured in “More Good News on Ivermectin.” Lawrie has now published her third systematic review. According to this paper, published June 17, 2021 in the American Journal of Therapeutics:8
“Meta-analysis of 15 trials found that ivermectin reduced risk of death compared to no ivermectin (average risk ratio 0.38 …) … Low-certainty evidence found that ivermectin prophylaxis reduced COVID-19 infection by an average 86% … Secondary outcomes provided less certain evidence.
Low-certainly evidence suggested that there may be no benefit with ivermectin for ‘need for mechanical ventilation,’ whereas effect estimates for ‘improvement’ and ‘deterioration’ clearly favored ivermectin use. Severe adverse events were rare among treatment trials …”
World Health Organization Refuses to Recommend Ivermectin
Despite the fact that most of the evidence favors ivermectin, when the WHO finally updated its guidance on ivermectin at the end of March 2021,9,10 they largely rejected it, saying more data are needed. They only recommend it for patients who are enrolled in a clinical trial.
Yet, they based their negative recommendation on a review that included just five studies, which still ended up showing a 72% reduction in deaths. What’s more, in the WHO’s summary of findings, they suddenly include data from seven studies, which combined show an 81% reduction in deaths. The confidence interval is also surprisingly high, with a 64% reduction in deaths on the low end, and 91% on the high end.
Even more remarkable, their absolute effect estimate for standard of care is 70 deaths per 1,000, compared to just 14 deaths per 1,000 when treating with ivermectin. That’s a reduction in deaths of 56 per 1,000 when using the drug. The confidence interval is between 44 and 63 fewer deaths per 1,000.
Despite that, the WHO refuses to recommend this drug for COVID-19. Rabindra Abeyasinghe, a WHO representative to the Philippines, commented that using ivermectin without “strong” evidence is “harmful” because it can give “false confidence” to the public.11
Why Ivermectin Has Been Censored
If you’ve been trying to share the good news about ivermectin, you’re undoubtedly noticed that doing so is incredibly difficult. Many social media companies are banning such posts outright.
Promoting ivermectin on YouTube, or even discussing benefits cited in published research, violates the platform’s posting policies. DarkHorse podcast host Bret Weinstein, Ph.D., is but one of the victims of this censorship policy.
His interviews with medical and scientific experts such as Dr. Pierre Kory, a lung and ICU specialist, former professor of medicine at St. Luke’s Aurora Medical Center in Milwaukee, Wisconsin, and the president and chief medical officer12 of the FLCCC, and Dr. Robert Malone, the inventor of the mRNA and DNA vaccine core platform technology,13 have been deleted from the platform. The interview with Malone had more than 587,330 views by the time it was wiped from YouTube.14
But why? Why don’t they want people to feel confident that there’s treatment out there and that COVID-19 is not the death sentence they’ve been led to believe it is? The short answer is because ivermectin threatens the vaccine program. As explained by Andrew Bannister in a May 12, 2021, Biz News article:15
“What if there was a cheap drug, so old its patent had expired, so safe that it’s on the WHO’s lists of Essential and Children’s Medicines, and used in mass drug administration rollouts?
What if it can be taken at home with the first signs COVID symptoms, given to those in close contact, and significantly reduce COVID disease progression and cases, and far fewer few people would need hospitalization?
The international vaccine rollout under Emergency Use Authorization (EUA) would legally have to be halted. For an EUA to be legal, ‘there must be no adequate, approved and available alternative to the candidate product for diagnosing, preventing or treating the disease or condition.’
The vaccines would only become legal once they passed level 4 trials and that certainly won’t happen in 2021 … The vaccine rollout, outside of trials, would become illegal.
The vaccine manufactures, having spent hundreds of million dollars developing and testing vaccines during a pandemic, would not see the $100bn they were expecting in 2021 … Allowing any existing drug, at this time, well into stage 3 trials, to challenge the legality of the EUA of vaccines, is not going to happen easily.”
The WHO and Drug Companies Are Severely Compromised
The WHO’s rejection of ivermectin only makes sense if a) you take into account the EUA requirements; and b) remember that the WHO receives a significant portion of its funding from private vaccine interests.
The Bill & Melinda Gates Foundation is the second largest funder of the WHO after the United States, and The GAVI Alliance, also owned by Gates, is the fourth largest donor. The GAVI Alliance exists solely to promote and profit from vaccines, and for several years, the WHO director-general, Tedros Adhanom Ghebreyesus, served on the GAVI board of directors.16
As reported by Bannister, Merck, the original patent holder of ivermectin, also has severe conflicts of interest that appear to have played a role in the rejection of ivermectin. He writes:17
“Ivermectin has been used in humans for 35 years and over 4 billion doses have been administered. Merck, the original patent holder,18 donated 3.7 billion doses to developing countries … Its safety is documented at doses twenty times the normal …
Merck’s patent on Ivermectin expired in 1996 and they produce less than 5% of global supply. In 2020 they were asked to assist in Nigerian and Japanese trials but declined both.
In 2021 Merck released a statement claiming that Ivermectin was not an effective treatment against Covid-19 and bizarrely claimed, ‘A concerning lack of safety data in the majority of studies’ of the drug they donated to be distributed in mass rollouts, by primary care workers, in mass campaigns, to millions in developing countries.
The media reported the Merck statement as a blinding truth without looking at the conflict of interests when days later, Merck received $356m from the US government to develop an investigational therapeutic.
The WHO even quoted Merck, as evidence, that it didn’t work, in their recommendation against the use of Ivermectin. It’s a dangerous world when corporate marketing determines public health policy.”
FLCCC Calls for Widespread and Early Use of Ivermectin
In the U.S., the FLCCC has been calling for widespread adoption of ivermectin, both as a prophylactic and for the treatment of all phases of COVID-19,19,20 and Kory has testified to the benefits of ivermectin before a number of COVID-19 panels, including the Senate Committee on Homeland Security and Governmental Affairs in December 202021 and the National Institutes of Health COVID-19 Treatment Guidelines Panel in January 2021.22
Based on a meta-analysis of 18 randomized controlled trials, ivermectin produces large statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance.
As noted by the FLCCC:23
“The data shows the ability of the drug Ivermectin to prevent COVID-19, to keep those with early symptoms from progressing to the hyper-inflammatory phase of the disease, and even to help critically ill patients recover.
… numerous clinical studies — including peer-reviewed randomized controlled trials — showed large magnitude benefits of Ivermectin in prophylaxis, early treatment and also in late-stage disease. Taken together … dozens of clinical trials that have now emerged from around the world are substantial enough to reliably assess clinical efficacy.”
The FLCCC has published three different COVID-19 protocols, all of which include the use of ivermectin:
I-MASK+24 — a prevention and early at-home treatment protocol
I-MATH+25 — an in-hospital treatment protocol. The clinical and scientific rationale for this protocol has been peer-reviewed and was published in the Journal of Intensive Care Medicine26 in mid-December 2020
I-RECOVER27 — a long-term management protocol for long-haul syndrome
In addition to Lawrie’s meta-analysis in the American Journal of Therapeutics, the FLCCC has also published a scientific review28 in that same journal.
This paper, “Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19,” published in the May/June 2021 issue, found that, based on a meta-analysis of 18 randomized controlled trials, ivermectin produces “large statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance.”
Ivermectin Significantly Reduces Infection Risk and Death
The FLCCC also found that when used as a preventive, ivermectin “significantly reduced risks of contracting COVID-19.” In one study, of those given a dose of 0.4 mg per kilo on Day 1 and a second dose on Day 7, only 2% tested positive for SARS-CoV-2, compared to 10% of controls who did not get the drug.
In another, family members of patients who had tested positive were given two doses of 0.25 mg/kg, 72 hours apart. At follow up two weeks later, only 7.4% of the exposed family members who took ivermectin tested positive, compared to 58.4% of those who did not take ivermectin.
In a third, which unfortunately was unblended, the difference between the two groups was even greater. Only 6.7% of the ivermectin group tested positive compared to 73.3% of controls. According to the FLCCC, “the difference between the two groups was so large and similar to the other prophylaxis trial results that confounders alone are unlikely to explain such a result.”
The FLCCC also points out that ivermectin distribution campaigns have resulted in “rapid population-wide decreases in morbidity and mortality,” which indicate that ivermectin is “effective in all phases of COVID-19.” For example, in Brazil, three regions distributed ivermectin to its residents, while at least six others did not. The difference in average weekly deaths is stark.
In Santa Catarina, average weekly deaths declined by 36% after two weeks of ivermectin distribution, whereas two neighboring regions in the South saw declines of just 3% and 5%. Amapa in the North saw a 75% decline, while the Amazonas had a 42% decline and Para saw an increase of 13%.
It’s worth noting that ivermectin’s effectiveness appears largely unaffected by variants, meaning it has worked on any and all variants that have so far popped up around the world. Additional evidence for ivermectin will hopefully come from the British PRINCIPLE trial,29 which began June 23, 2021. Ivermectin will be evaluated as an outpatient treatment in this study, which will be the largest clinical trial to date.
Ivermectin in the Treatment of Long-Haul Syndrome
The FLCCC believes ivermectin may also be an important treatment adjunct for long-haul COVID syndrome. In their June 16, 2021, video update, the team reviewed the newly released I-RECOVER protocol.
Keep in mind that ivermectin is not to be used in isolation. Corticosteroids, for example, are often a crucial treatment component when organizing pneumonia-related lung damage is present. Vitamin C is also important to combat inflammation. Be sure to work with your doctor to identify the right combination of drugs and supplements for you.
Last but not least, as noted by Kory in this video, it’s really important to realize that long-haul syndrome is entirely preventable. The key is early treatment when you develop symptoms of COVID-19.
While ivermectin has a good track record when it comes to prevention and early treatment, it can be tricky to obtain, depending on where you live and who your doctor is.
A highly effective alternative that anyone can use, anywhere, is nebulized hydrogen peroxide. It’s extremely safe and very inexpensive. The biggest cost is the one-time purchase of a good tabletop jet nebulizer. To learn more, download Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery,” in which he details how to use this treatment.
It’s as ‘safe & effective’ as can be says the NZ government, whose Doctors are not allowed to fully inform you of any downside type reactions. Like death for instance. Or stroke or cardiac arrest. If they did, well you might decide not to take it.
FYI I’ve added below the full list of possible adverse events from the FDA website, all links provided so you can read for yourself as your rights to do so shrink rapidly before your eyes. EWR
Two sources, the odysee should work … it’s reported the fb one doesn’t although it works for me:
You aren’t necessarily going to get all of those or even any of them if you have the vaccine. But those are the possible side effects that the FDA has listed. They’re all unpleasant, most of them very serious and you can’t get more serious than death. Below are the deaths & injuries reported to the official government data bases that occurred after taking the covid-19 injection. Remember only 1% on average are reporting.
CURRENT DEATH & INJURY STATS REPORTED: (links to reporting sites below)
USA: DEATHS – 4,863 INJURIES: 262,521 (to June 24 )
UK: 1,295 DEATHS – INJURIES 922,596 (to June 10th)
EUROPE: 13,867 – INJURIES 1,354,336 (to June 5th)
AUSTRALIA – 210 DEATHS – 22031 INJURIES (to 27 May)
As infectious disease epidemiologists and public health scientists we have grave concerns about the damaging physical and mental health impacts of the prevailing COVID-19 policies, and recommend an approach we call Focused Protection.
After being in the “hesitant” category for several months I am now in the “no” category. As a retired medical doctor I have plenty of time, and a genuine fascination, to thoroughly research this topic. I have been diligently reviewing every scientific journal I can find, reading every online news article I come across, and going through countless case reports on the CDC VAERS website. I now have a clearer understanding of how these vaccines influence our immune system and organs, how they could be of benefit, and how they cause the multiple short, medium, and long term adverse effects.
I am convinced that the benefits promoted by experts on TV regarding these vaccines are less than what they promise, and the adverse reactions are more than they want us to believe. The effects of these vaccines on the human body are infinetely more complex than anyone can imagine… a million shades of gray, you may say.
A few friends have asked my thoughts on the covid jab(s) so I thought it was time to write an article on the topic.
All my friends had not heard most of the details I shared, so I figured you might appreciate hearing some of what I told them.
Knowing how contentious this issue is, part of me would rather just write about something else, but I feel like the discussion/news is so one-sided that I should speak up.
As I always strive to do, I promise to do my best to be level-headed and non-hysterical.
I’m not here to pick a fight with anyone, just to walk you through some of what I’ve read, my lingering questions, and explain why I can’t make sense of these covid vaccines.
Evidence suggests people who have received the COVID “vaccine” may have a reduced lifespan as a result of the acute, subacute and long-term effects from the COVID injection
If you’ve gotten the COVID shot, consider yourself high risk for COVID and implement a daily prophylaxis protocol. This means optimizing your metabolic flexibility, vitamin D, and taking vitamin C, zinc and a zinc ionophore on a daily basis, at least throughout cold and flu season
Evidence shows NAC may be used to prevent blood clots and break up any that might already have formed
If you’re low risk for COVID and have not been vaccinated, make sure you have these items on hand and begin treating at the very first signs of cold or flu symptoms
Also buy yourself a tabletop jet nebulizer, some saline solution and food grade hydrogen peroxide. Nebulized peroxide is an excellent go-to both for prevention and treatment, regardless of the stage the respiratory infection is in. For prevention, nebulize every other day. For treatment, use at first signs of respiratory infection
In this interview, return guest Dr. Vladimir Zelenko discusses an incredibly serious concern, one shared with at least two other highly credible experts — Michael Yeadon, Ph.D., a life science researcher and former vice-president and chief scientist of allergy and respiratory research at Pfizer, and professor Luc Montagnier, a world-renowned virologist who won the Nobel prize for his discovery of HIV.
Yeadon, Montagnier and Zelenko all believe the COVID-19 shots could reduce life expectancy by several decades, depending on several factors, including whether you’re required to get booster shots. In fact, there may be reason to suspect that many who get the jabs and subsequent boosters could lose their lives within two to three years, as a result of pathogenic priming.1,2
Many may not realize that when I was a youngster I was a Boy Scout, but you might know their motto is “Be Prepared.” It is an approach that has served me well over the years. I am not stating unequivocally that dire outcome will materialize, as my interview next week with Dr. Peter McCullough goes into. However, it would seem prudent to have a good protocol in your hands in anticipation of a worst-case scenario.
So, on that note, Zelenko and I take a deep dive into what can be done to prevent such a fate. Zelenko categorizes the risks of COVID-19 “vaccines” into three categories: acute, subacute and long-term, so let’s begin by reviewing the primary risks found in each of these categories.
Risk Category No. 1 — Acute Risks
The acute phase of harm begins at the moment of injection and likely lasts for about three months or so. Based on reports filed with the U.S. Vaccine Adverse Event Reporting System (VAERS), it’s clear that many cannot survive past the acute phase.
About 6,000 deaths have been reported so far, and death commonly occurs within 48 hours of injection. Many serious disabling events also occur rather rapidly, typically within a few days or weeks. However, Zelenko has a very dismal perspective on the accuracy of the VAERS database. He explains:
“According to a paper published by the Salk Institute in San Diego, they’ve discovered that the spike protein that’s generated through the vaccination itself has negative health effects. It’s toxic … on its own …
There’s plenty of evidence that shows that it spreads from the injection site and goes to the bloodstream, and basically comes into every single cell in the body.3,4
mRNA has a half-life of around one to two weeks, depending on the mRNA, and during that interim, each mRNA molecule makes around 2,000 to 5,000 spike proteins. So, we’re talking about trillions and trillions of spike proteins.
Your entire body becomes a spike protein factory. Several orders of magnitude more than if you were to get COVID, because COVID infects the upper and lower airways primarily. Those are the cells that get infected and begin to produce spike proteins. But here we’re injecting the vaccine and it actually travels to every single cell in your body and converts every single cell in your body into a factory for spike proteins.”
As the mRNA disseminates through your vascular system, the cells lining your blood vessels begin producing spike protein. This is why we’re seeing such a staggering number of reports of people experiencing blood clots from these injections.
According to Zelenko, 40% of these events occur within the first two days after injection. The risk then diminishes, but vascular events such as heart attacks, strokes, renal infarcts and pulmonary infarcts don’t completely peter out until about three months after the last injection.
But these events of the past three months are not being reported to VAERS. It is, of course, possible that people simply aren’t connecting them to the COVID shot they got several months earlier.
How Many Have Actually Died From the COVID Shots?
As noted by Zelenko, underreporting is part of the problem we’re facing. The real number of side effects is impossible to determine, given the fact that the Food and Drug Administration didn’t insist on a robust post-vaccination data collection system, but it’s most certainly higher than what VAERS is listing.
“If you look at the VAERS [vaccine adverse event reporting system], which in my opinion is a piece of garbage … as of today, let’s say says there’s 6,000 deaths associated with taking the vaccine. Well, we need to understand what that actually means,” Zelenko says.
“If you look at the 2009 Harvard study on the VAERS system, they said only 1% of events are actually reported. So, OK … whatever the number is, it’s not 6,000. Maybe only 10% are being reported. I don’t know. But definitely it’s being underreported.
And then there’s two [additional] big problems. There’s evidence coming out that VAERS reports that have been filed are being erased off the server, No. 1. No. 2, I personally know of two dozen cases of deaths associated with the vaccine, and the doctor and/or family members that tried to file a VAERS report, their reports were rejected due to some technicality.
The fact that they all couldn’t make a report, that raises my eyebrows. What percentage of the information are we actually seeing? The answer is, I estimate, there are already around 200,000 dead Americans, directly related to the vaccinations.”
To get to that number, Zelenko assumes only 10%5 of adverse effects are reported. Studies have indicated it could be as low as 1%.6,7 That gives us a death toll of about 60,000, to which he adds another 140,000 given the fact that reports are being scrubbed and refused.
“The point is that it should definitely raise eyebrows and have the public start screaming and saying, ‘We want to know the truth. We want to know the accurate numbers. Stop suppressing the truth … I want to be able to make an informed choice whether or not I want to take this injection.’ And that’s not being given to the people.
My problem is not with the vaccine. My problem is with the government, governing bodies and certain people that are obstructing the flow of life saving information and suppressing the truth from people, and then using coercion to force people to take this vaccine. That’s the nefarious part.
The suppression is so blatant and so overt that doctors with impeccable credentials are being deplatformed for just voicing an opinion. And then you couple that together with proven prehospital treatment approaches and protocols that have been proven to reduce hospitalization and death by 85%, and that information is being suppressed.
So here you have a dual censorship where the positive, hopeful, life-saving information is being suppressed and the dangerous outcomes of the vaccination approach is being suppressed. It’s a perfect setup for genocide.”
Risk Category No. 2 — Subacute Risks
The subacute risk phase, which begins around three months’ post-injection, is exceedingly difficult to quantify. At bare minimum, it’s likely to last several months to a couple of years. The primary concern now is antibody-dependent enhancement (ADE), also referred to as pathogenic priming and/or paradoxical immune enhancement (PIE) as it more accurately describes the disease mechanism.
Zelenko believes the mRNA will have degraded by this time, and your cells will hopefully no longer produce spike protein. I believe he may be overly optimistic here, as the synthetic mRNA has been genetically modified to be less perishable, plus it’s encased in a nanolipid to resist breakdown.
I suspect this modified mRNA may remain viable far longer than anyone suspects, thanks to its synthetic nature. What’s more, there’s a mechanism by which the mRNA can be reverse transcribed into your DNA, which would make the spike protein production permanent — and probably intergenerational. I describe this process in “The Many Ways in Which COVID Vaccines May Harm Your Health.”
If Zelenko is correct, then the primary disease agent now switches from the spike protein to the antibodies produced in response to the spike protein. We don’t know how long these antibodies will last, but chances are they’ll stick around for a number of months or years.
While antibody production is the primary purpose of these shots, and the response said to provide you an immune benefit, they can actually be the source of problems.
Animal trials in which conventional coronavirus vaccines were tested have shown coronavirus vaccines routinely cause ADE,8,9,10,11,12 so when the animals are challenged with the real virus they’ve been immunized against, they can get seriously ill and even die. If hospitals start filling up with vaccinated individuals this fall, you’ll know why. They’re suffering the effects of ADE.
“In other words, those antibodies that were produced with the vaccination were pathologic,” Zelenko says. “They were lethal and they led to an exaggerated immune response. That’s what it means, antibody-dependent enhancement. It’s an enhancement of your immune response in a way that it will kill you …
The question is, how safe is it long-term, or in the subacute [phase] from three months to three years? That is a big question mark. Based on animal models — and this is what Dr. Mike Yeadon is saying — it could be absolutely genocidal. It’s the biggest gamble on the survival of humanity in the history of humanity.”
However, as a counter to this view, Dr. Peter McCullough, who is in complete agreement with the engineering of this event and it being one of the most egregious crimes against humanity, is not convinced that there will be a massive die-off in the fall.
He is well-trained in the science and has essentially completed a fellowship in COVID-19 along with being the senior editor of two prestigious medical journals so his opinion also deserves consideration. We will be posting his interview next Sunday, July 11, 2021.
Why Is Humanity’s Survival Being Risked?
The questions on many people’s mind right now are, “Why are lifesaving early treatment approaches suppressed?” “Why are the toxic side effects and death rates of the vaccines being suppressed?” and “Why are entire continents being coerced into taking a vaccine that is both medically unnecessary and unproven in terms of safety and effectiveness?”
Taken together, none of it makes any sense, which is why people like Yeadon, Montagnier, Zelenko and others are raising concerns about global genocide. Is that what this is all about? Is there an alternative interpretation of what’s happening? When you consider the actual data, mass vaccination simply isn’t necessary, so why the frantic push to get a needle in every arm? Zelenko explains:
“There’s something called medical necessity. So, let’s analyze if there’s any medical necessity for this vaccine, and you have to do that in a systematic way based on demographics.
If you look at the CDC’s data, anyone 18 and younger has a 99.998% chance of recovery from COVID-19 with no treatment. [Their risk of dying is] 1 in a million. It’s safer than influenza virus. If you gave me a choice, I would rather my kids have COVID-19 than influenza. So, why would I immunize a demographic that has close to 100% chance of recovery with an experimental vaccine that has already killed more kids than the virus?
If you look at the demographic between 18 and 45, people who are healthy have a 99.95% chance of recovery with no treatment … according to the CDC. Same question, why would I vaccinate a demographic that recovers on its own with no treatment?
Third question, if someone has antibodies — and there’s a plethora of evidence [showing] naturally produced antibodies are much more effective in clearing future viruses than vaccine-induced antibodies … Natural immunity is much better, more effective and safer, than vaccine-induced immunity. So, someone who has antibodies already from having COVID before, why would I vaccinate them? …
Fear is an extremely useful tool in manipulating the behavior of people. And that fear has been used to create a psychological motivation to get vaccinated with a vaccine that, in my opinion, has no medical necessity, has tremendous amount of actual and potential risks, and very questionable efficacy.”
Risk Category No. 3 — Long-Term Risks
Beyond the two-to three-year mark are the long-term risks, which are even more difficult to predict. One particularly difficult risk to predict or quantify is infertility. It’ll take decades before we have the data on reproductive effects. Women in their 20s who get the jab might not get serious about trying to get pregnant until they’re in their 30s.
Teens and young children will have to wait decades before fertility can be ascertained. Of course, by then, it’ll be too late. The damage will be done, and hundreds of millions will be in the same boat.
Zelenko cites research published in The New England Journal of Medicine, which concluded COVID vaccination during pregnancy had no increased risk of miscarriage. However, a closer look at the data set revealed that this was only true for women who got vaccinated during their third trimester. Women who get the COVID jab in their first and second trimester have a 24-fold higher risk of miscarriage.
There are also reports of declining sperm counts and testicular swelling in men, and menstrual cycle disruptions in women of all ages. “There is an absolute effect on fertility,” Zelenko says. We just don’t know to what degree yet.
Overall life expectancy is likely to be affected across the board but, again, it’s very difficult to predict just how many years or decades will be lost. Zelenko, like many other doctors, suspect autoimmune diseases and cancer rates will go up as a result of the jabs. As noted by Zelenko:
“Whether you look at the acute spike protein-induced death, the miscarriages, or the myocarditis in young adults, or you look at the subacute pathogenic priming issue, or you look at the potential long-term effects of infertility, auto immune disease and cancer, you have an absolute setup for a genocide. And that’s why these world-leading thought leaders, scientists, are cautioning people …
Let’s do a thought experiment. If COVID-19 were to infect every single human being on this planet and was not to be treated, what would be the overall global death rate? The answer is less than 1%, and I’m not advocating for that, by the way. That’s a lot of people still.
Now, what is going to be the death rate from global vaccination? That is going to be several orders of magnitude greater. And it actually depends how far out you look. Because if someone’s meant to live 80 years and they live 60 years, how do you quantify that? …
We’re talking about 1.5 to 2 billion people [dying] for no reason, except the agendas of a few psychopaths or sociopaths. Why do I say that? It’s because there have been people advocating for population reduction for decades. I just saw a video from [U.K. prime minister] Boris Johnson’s father … advocating for the reduction of England’s population to 15 million …
This type of ideology exists. In this generation, it’s not really anti-Semitic. What it is, is there’s a small group of sociopaths that believe … they’ve evolved into a superhuman enlightened [state] that entitles them the right to dictate the course of history.
For example, Bill Gates in 2015 said the world population needs to be reduced by a certain percentage because of global warming or whatever. So, my question is a very simple question. He’s one of the main supporters and profiteers of global vaccination. Why would I take a vaccine for my health from someone is advocating for the reduction of the world population?
Another scary individual is Klaus Schwab, the founder of the World Economic Forum. He’s very influential. He wrote the book ‘COVID-19 The Great Reset.’ In 2016, in a French interview … Schwab made an announcement that within 10 years, all of humanity will be tagged with an identifier. If you look at the UN 2030 plan, which was crafted by the World Economic Forum, it says ‘America will no longer be a superpower.’
That’s a stated agenda. Then, my favorite is, ‘You’ll own nothing and you’ll be happy. You won’t eat any meat. Fossil fuels will be prohibited. There’ll be a billion refugees, which will have to be integrated into your societies.’ So, my question is, what sociopath feels entitled to make a statement like ‘You will own nothing and you will be happy’?
What entitles this type of individual, or group of individuals, to think that way? Well, they believe that they’re enlightened far beyond the average human or subhuman.”
War Against God
Zelenko, a devout Jew, believes the root of this global takeover is really a war against God. The implication is that life has sanctity, and if life has sanctity, we have human rights, “earned” by our birth alone. This is the source of natural law. And, if we have human rights, handed down by God, then no one has the right to decide how long any one of us should live, or how many people there should be on the planet.
“That’s God’s prerogative,” Zelenko says. “However, if you take that out and view people as no different than an animal, a Darwinist perspective or eugenics perspective, and basically survival of the fittest is the yardstick that you measure the dominance hierarchy of humanity, in that case, these people feel that they are on top of the pyramid, and that entitles them to decide if you and me should live …
I call the [COVID] vaccine ‘Zyklon-V.’ That is the gas the Nazis used to kill my relatives. So to express my sentiments, I call it Zyklon-V. It’s an absolute weapon of mass destruction. People are being lied to, and they’re running into the gas chambers themselves because of the pathogenic fear.”
How to Protect Your Health Post-Jab
If you or someone you know or love got the COVID jab and now have serious regrets, there are definite strategies you can use to protect your health.
It appears if you made it through the first three months OK, then your risk for blood clots is likely radically diminished. To counteract excessive clotting, an anticoagulant may be appropriate. A natural alternative with great promise is n-acetyl cysteine (NAC), as it has both anticoagulant13 and thrombolytic effects,14 meaning it may both prevent clots and break up clots that have already formed. Obviously, do not get any more booster shots.
In the subacute phase, your No. 1 goal will be to avoid ADE. The key to this is to avoid triggering a pathogenic immune reaction, and the only way to do that is to implement some sort of prophylactic protocol, i.e., a COVID, common cold and influenza prevention protocol.
This is especially important for anyone that has received the COVID jab as they are at a high risk of having complications and are under the false impression that they are “protected” when actually they are at increased risk now that they got the jab and need to take extraordinary precautions.
Any symptoms of upper respiratory infection should also be treated immediately, not later. COVID is a multi-phase disease. The first phase is the viral phase, which lasts five to seven days. This is when it’s most easily treated. After Day 7, the disease typically progresses into the inflammatory phase, which requires different treatment.
Zinc supplementation is an important component for prevention and early treatment in the viral stage, as it impairs viral replication. You need to take it with a zinc ionophore, however, such as quercetin, EGCG (green tea extract), hydroxychloroquine or ivermectin.
“The majority of the COVID protocols focus on inhibition of our RNA virus replication. What that means is that for a virus to make copies of itself, it needs to enter the human cell. In the case of RNA viruses, all the COVID, coronaviruses and even the influenza viruses, they use a common pathway called RNA dependent RNA polymerase. That’s a very important enzyme.
That enzyme is what makes copies of the viral genetic material, which then enables for new viruses to be formed and spread. So, if you inhibit the viral RNA replication process, you’ll eliminate viral spreading, viral growth. The beautiful thing about what we found with zinc is that zinc inhibits this enzyme extremely well, if there’s another zinc [molecule] inside the cell.
But zinc cannot really get into the cell on its own. That’s where the concept of zinc ionophores come in. Zinc ionophores opens the door in the cell membrane and allows for zinc to go from outside of the cell, to inside of the cell. And when you increase the concentration of zinc inside the cell, then it can effectively inhibit this enzyme, stopping most if not all, coronaviruses and influenza viruses from replicating.”
If you want to use either hydroxychloroquine or ivermectin and live in a state that restricts their use, look for online telehealth options. The American Frontline Doctors is one resource. They only charge $90 for a consultation and you will be able to get the prescription that you need. Do not use Ivermectin from veterinary sources as it may be contaminated and is not designed for human use.
If you’ve gotten the jab, consider yourself high risk for COVID and implement a daily prophylaxis protocol. This means optimizing your vitamin D, and taking vitamin C, zinc and a zinc ionophore on a daily basis, at least throughout cold and flu season.
In addition to zinc and a zinc ionophore, you also need to optimize your vitamin D level. The range you’re looking for is 60 ng/mL to 80 ng/mL year-round. The appropriate dose of oral vitamin D3 is the dose that gets you within that range.
Vitamin C is another important component, especially if you’re taking quercetin, as they have synergistic effects. To effectively act as a zinc ionophore, the quercetin needs vitamin C.
In an effort to make it easier for patients, Zelenko has developed an oral supplement that contains all four: vitamin C, quercetin, vitamin D3 and zinc. It’s called Z-Stack and can be purchased on zstacklife.com. For a downloadable “cheat sheet” of Zelenko’s protocol for COVID-19, visit VladimirZelenkoMD.com
The take-home message here is that if you’ve gotten the jab, consider yourself high risk for COVID and implement a daily prophylaxis protocol. This means optimizing your vitamin D, and taking vitamin C, zinc and a zinc ionophore on a daily basis, at least throughout cold and flu season.
It would also be useful to do a daily sauna. Ideally one that can heat up to 170 degrees Fahrenheit. The best saunas are far-infrared and have low EMFs. Sadly, I don’t know any that go to 170 degrees and are low EMF.
I use one that goes to 170 and then I turn it off and turn on the SaunaSpace four near IR bulb system in the sauna and go in for 20 minutes. This practice activates heat shock proteins which will help remove the spike proteins and improve other damaged proteins in your body.
If you’re low risk for COVID and have not been vaccinated, make sure you have these items on hand and begin treating at the very first signs of cold or flu symptoms.
Strategies to Lower Risk in Those Who Received COVID Jab
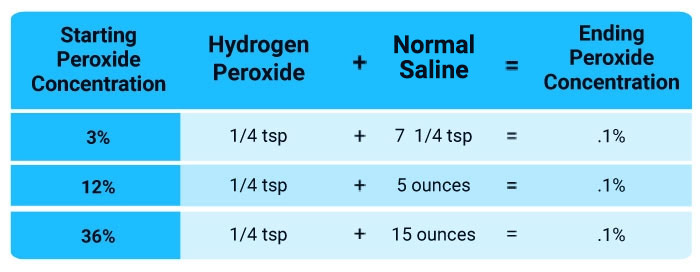
Nebulized hydrogen peroxide 0.1%
Daily or more frequently if needed
NAC (N-acetyl Cysteine)
500 mg once a day
Zinc
15 mg once a day
Vitamin C
500 mg once a day or 250 mg twice a day
Eliminate ALL vegetable (seed) oils
Goal is zero
Vitamin D
Most adults need 8000 IU per day but it is imperative to check blood levels 60-80 ng/ml or 100-150 nmol/l
Daily sauna
20 minutes at 170 degrees will help destroy spike proteins
Time restricted eating
Helps remove spike proteins through autophagy
Seek to eat organic only foods, especially avoid the dirty dozen
This will help limit glyphosate intake
Nebulized Peroxide and Other Health Promoting Measures
In addition to NAC (to prevent and break up clots), vitamin D, vitamin C, quercetin and zinc, buy yourself a tabletop jet nebulizer, some saline solution and food grade hydrogen peroxide. You’ll want to dilute the peroxide with saline to get a 0.1% solution.
Nebulized peroxide is my personal go-to both for prevention and treatment, regardless of the stage the respiratory infection is in. To learn more, download Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.” As a preventive measure, simply nebulize every other day. Vitamin C is important here too, as it works as a catalyst for the peroxide. A daily dose of 500 milligrams would likely be sufficient for most.
We were forced to remove all the hydrogen peroxide videos that I had previously posted for liability reasons but fortunately they are all now posted on our Substack site. This is important as, in my view, this is the most important step you can take. I would recommend nebulizing a 0.1% solution every day as indicated in the videos, linked below.
There is no danger in doing it every day and likely there is a health benefit. As Dr. Tom Levy describes in one of the videos below, it seems to help improve your bowel movements, which may be a result of eliminating respiratory pathogens that were having negative impact on your microbiome.
Other important health-preserving strategies include the following:
• Make sure you’re metabolically flexible so that your body can seamlessly transition between burning fat and sugar as your primary fuel. This will allow your innate immune system to function optimally. Time-restricted eating is one surefire way to accomplish this.
• Avoid processed seed oils in your diet, such as sunflower oil, corn oil, safflower oil or avocado oils. All contain high levels of linoleic acid, which impairs your mitochondrial function, and in upper respiratory infections, it’s the precursor for the Leukotoxin that occurs in these infections.
• Focus on certified-organic foods to minimize your glyphosate exposure, and include plenty of sulfur-rich foods to keep your mitochondria and lysosomes healthy. Both are important for the clearing of cellular debris, including these spike proteins. You can also boost your sulfate by taking Epsom salt baths.
• To combat the toxicity of the spike protein, you’ll want to optimize autophagy, as this may help digest and remove the spike proteins. Time-restricted eating will upregulate autophagy, while sauna therapy, which upregulates heat shock proteins, will help refold misfolded proteins. They also tag damaged proteins and target them for removal.
It is important that your sauna is hot enough (around 170 degrees Fahrenheit) and does not have high magnetic or electric fields.
• If you’re having post-vaccination symptoms, you could consider:
◦ Low-dose interferons such as Paximune, to stimulate your immune system
◦ Peptide T (an HIV entry inhibitor derived from the HIV envelope protein gp120; it blocks binding and infection of viruses that use the CCR5 receptor to infect cells)
◦ Cannabis, to strengthen Type I interferon pathways, which are part of your first line of defense against pathogens
◦ Dimethylglycine or betaine (trimethylglycine) to enhance methylation, thereby suppressing latent viruses
◦ Silymarin or milk thistle to help cleanse your liver
Of the 700 physicians responding to an internet survey by the Association of American Physicians and Surgeons (AAPS), nearly 60% said they were not “fully vaccinated” against COVID, according to a press release from PR Newswire.
This contradicts an American Medical Association claim — based on 300 respondents — that 96% of practicing physicians are fully vaccinated. Neither survey is representative of all U.S. physicians, but the AAPS survey shows that support among doctors for the COVID injection campaign is far from unanimous.
The AAPS survey also showed that more than half of physician respondents were aware of patients suffering a “significant adverse reaction.” Of the unvaccinated physicians, 80% said “I believe risk of shots exceeds risk of disease,” and 30% said, “I already had COVID.”
“It is wrong to call a person who declines a shot an ‘anti-vaxxer,’ ” AAPS executive director Dr. Jane Orient said. “Virtually no physicians are ‘anti-antibiotics’ or ‘anti-surgery,’ whereas all are opposed to treatments that they think are unnecessary, more likely to harm than to benefit an individual patient, or inadequately tested.”
She went on to say that causality is not proven. “However,” she said, “many of these episodes might have resulted in a huge product liability or malpractice award if they had occurred after a new drug, but purveyors of these COVID products are protected against lawsuits.”
In a week of very worrying developments, HART has been particularly appalled by a recent piece on BBC Newsround promoting the Pfizer vaccine for children.
HART’s most senior doctors are in full agreement that this video material is heavily biased, makes a series of factually incorrect statements, could be considered coercive propaganda and likely breaches the marketing authorisation. It is particularly concerning that the main speaker in the piece – a public health academic – is not a qualified clinician.
Of even greater concern, we are aware that it has been shown in schools. The bottom line is this: children are essentially at zero risk of COVID-19. Any justification for the vaccination of children must therefore be able to prove unequivocally that the cure is not worse than the disease.













![On the NZ [‘unofficial’ CV VX] front, a death & an adverse event](https://envirowatchnz.com/wp-content/uploads/2021/05/copy-of-death-2421820_1280.jpg?w=672&h=372&crop=1)
















You must be logged in to post a comment.