The Origins of the NZ Government’s Covid Elimination Strategy, Lockdown Laws and Mass Vaccination Drive
The origins of the New Zealand Government’s elimination strategy is traced, as well as its aspiration for high vaccination uptake and the nation’s embroilment in the World Health Organization’s pandemic trigger mechanisms — back to a 2002 Ministry of Health discussion paper published, as the SARS-Cov-1 outbreak began.
As far back as 2005, the United Nations’ World Health Organisation gained the power to construct trigger mechanisms to declare pandemics, that would eventually lead to the health departments across the 196 members nations being reoriented for an over-hyped health crisis.
Former news and current affairs editorSteve Snoopman finds that New Zealand’s Government gained for itself invasive powers to lockdown, search, seize and detain with amendments to the Public Health in 2006. Yet, the Government has exploited the over-hyped Covid-19 hysteria to expand its Medical Martial Law powers.
New Zealand’s Stealthy Pivot to Police State Status — Part 2
Lying by Numbers, Hyped Fear-Porn News and the U.N.’s 2nd Global Pandemic Exercise, starring ❛Covid-19❜
New Zealand’s response to the Covid-19 pandemic was (and remains) disproportionate to the threat because the Government failed to model for the United Nation’s Second Global Pandemic Exercise being taken ‘live’ — amid a planned media hype strategy. This failure was ‘too stupid to be stupid’.
The latest Covid-19 lockdown of the entire nation — which was announced on August 17 and was initially justified on the basis of just one suspected Delta variant case — actually followed a government commissioned report released the previous week that warned of the impacts of the Delta variant spreading from other countries, including Australia.
However, this investigation finds that despite the media hype of the Delta variant mortality, the figures from overseas do not wear the fear.
NZ Health Group managed to continue profitable business during 2021-22 when all 2467 ‘vaccine’ mandate exemption applications for their staff were granted by the (anon) Gov Covid Exemption Panel.
I’ve written before about the NZ ‘vaccine’ mandates and exemptions. An overview is here, and here and more specifically I’ve looked at many of the impacted public sector workers, like the nurses,teachers, paramedics and also in our prisons. I’ve also written a lot about ways academia controls the narrative, which include the revolving doors of international Public Private Partnerships (PPPs). Here, I want to focus on an example of how all these topics – academia, PPPs and wealthy shareholders – fit together.
Re-Cap on ‘No Jab, No Job’
During the height of the covid era totalitarianism, it was virtually impossible for any public (or commercial) sector worker who was mandated, to obtain an official ‘exemption’. Like many stories around the globe, whether your application was based on health, cultural or religious grounds, ALL were dismissed in the unethical and illogical claim:
“It’s for the Greater Good”
Many of us already knew the mandates were anti-science, but it became more widely known in MEP Robert Roos’ great Tweet when Pfizer exec Janice Small sniggered as she confirmed the fact there was no testing for transmission (45 secs):
Health Forum NZ, the Nurses’ Professional Association of New Zealand, NZDSOS and NZTSOS and many other such national advocacy groups have pointed out, the gatekeepers of the schools, prisons, surgeries, universities, hospitals and so many other organisations, including the unions, prevented staff from even knowing what the procedures for applying for an exemption were, let alone submitting one on their behalf. As a direct result of this blanket policy and military-grade censorship and propaganda, many people understandably felt coerced or forced to get the jab, and were subsequently harmed, or even died as a result.
Exemptions were literally SO rare (even those who had taken one dose and suffered an adverse reaction, were tragically not exempted from having to get a second, or third), that many people assumed no-one managed to avoid the wrath of the BigPharma captured Ministry of Health diktat.
But then I discovered that at least 6,707 healthcare-related staff in NZ were granted an exemption to the mandate under the law. (This has now been revised to 5,216 – more on that soon). So I was intrigued to find out who these people were – and more importantly, how these exemptions were obtained.
It turns out, after complaining to the Government Ombudsman, in a long-awaited OIA response that I sent 11 October 2023 (Ref HNZ00030952), that 11,741 total applications for ‘vaccine’ mandate exemptions were received between 27 Oct 2021 and 5 Sept 2022.
Gold Dust Exemptions
Amongst the long spreadsheet of redacted items, one thing stands out: the repeated applications for multiple individuals (some will be duplicates for extensions) from the commercial entity ‘New Zealand Health Group’. The main shareholder, NZ-Rich Listed Doug Catley’s empire has accumulated many names (see the image below). All are involved in providing some type of community-level care for our diverse population, from mental health counselling, agency staffing or emergency alarms etc:
According to its website, New Zealand Health Group is the
“largest community health, disability and wellbeing group supporting over 30,000 people to get on with making the most of life in their own homes, communities and work places…”
And at the helm, CEO since last year is Jane Kelley. What was she doing prior to Jan 2023 you ask? Well, it won’t be any surprise to those familiar with the revolving doors of power, that she was at the NZ Ministry of Health as ‘Director, National Controller’ for the ‘Covid-19 National Health Coordination Centre’.
“Addressing the workforce shortage is an example of progressive collaboration. Working in partnership with MSD (Ministry of Social Development), we have successfully trained and employed more than 1000 new support workers, some who (sic) may not have considered the home and community sector a viable employment option. We’ve also set up programmes that enable people who are helping care for family and whānau at home, to use their skills to qualify as a support worker.” (my emphasis)
The ‘beauty’ of the PPPs (for people like Kelley) is that any detail about the funds collected by these ‘partnerships’ with MSD etc are outside the Official Information Act (OIA), and any questions to the Gov Dept concerned are often bounced back with the claim “commercially sensitive”. Hence the true extent of the exploitation and profits that Health Group NZ makes from tax-payers’ funds being syphoned into ambiguously defined ‘care’, is unknown. This is a global problem as PPPs and their leeches have grown in the impact investor financial sector.
Likewise, OIAs have failed to get any transparency about who exactly the people were at the top of the NZ Gov ‘Covid Response’ decision-making (apparently due to Privacy Act reasons). But it’s useful to investigate who this Panel MAY have included.
Looking at Kelley’s public career profile for a moment, we can see her Linkedin page lists her most recent appointment as beginning in Nov 2022, which supports this PR-firm’s announcement (stating she actually started her role in January 2023), which goes on to state:
With over 25 years in the health sector, Jane has held a variety of executive, operational, and project leadership roles. Most recently Jane was the Director – National Controller Covid19 – National Health Coordination Centre, responsible for facilitating the Ministry of Health’s initial crisis response to Covid19. This was a pivotal role that involved establishing and leading a team of 300 and developing strategic relationships with multiple stakeholders from the highest level in Government through to local communities.
I wonder who her ‘team of 300’ were? Any Whistleblowers amongst them perhaps? But this same article is bending the truth slightly, claiming that her ‘most recent’ role was at the Ministry of Health – or was it? Let’s look more closely at her Linkedin profile (screenshot below):
“Business Change/Policy, Research and Development/Procurement and Logistics”
This status means it can effectively fast-track through any NZ Government tender process to obtain potentially lucrative funding/contracts. That doesn’t seem like a good idea to me as a NZ taxpayer, but it’s the ‘new normal’ of the PPP impact investment world.
Screenshot from the NZ Health Group website (as at 18/03/2024)
The Fernhill Solutions website is (conveniently) down at the time of writing this. But back in 30 January 2021 Kelley was indeed listed on the ‘Our People’ section of the archived version of their website along with David Crowley. But upon further investigation at NZ Companies Services, we can see the new shareholding company of Fernhill Solutions ‘Hapuna Holdings’, with Crowley and Kelley also as Directors. (They are also Directors of Hapuna Equine and Hapuna Developments). One of the last items posted on the Fernhill Solutions website is this poorly-written article (eg ‘Addition’ in the first line should read ‘Addiction’) about collating Public Submissions for a Report to Government…
Screenshot of the WayBack Machine capture from the Fernhill post (Jan 2020)
Up until Aug 2020, Kelley was apparently also a Director of Avid Support Ltd, a H&S consultancy business, based in Dunedin.
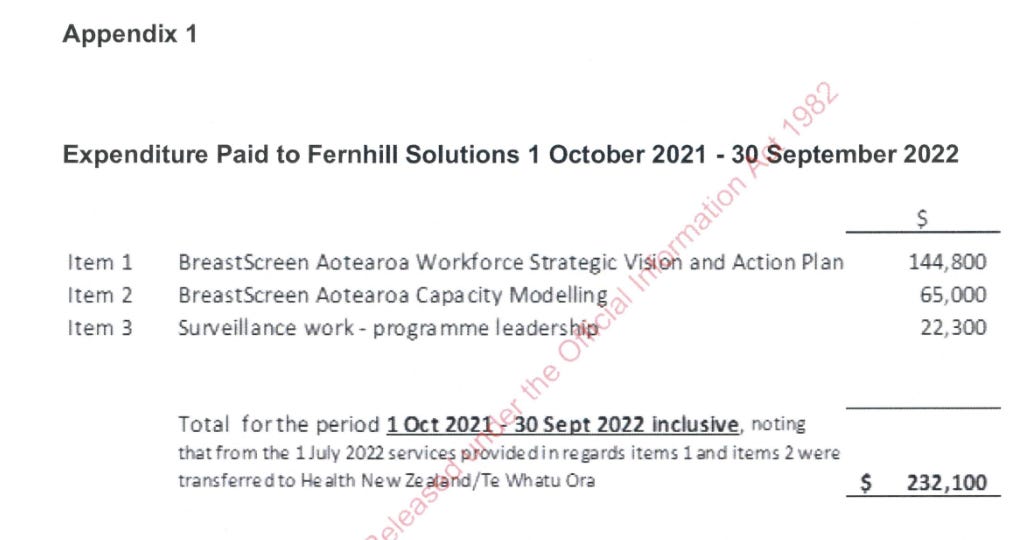
Edit to add an Addendum here 28/05/24. OIA responses have revealed that Kelley’s Fernhill Consultants were paid by NZ Government a total NZ$232,100 during the height of the covid era (mandate) insanity (Oct 2021-Sept 2022). Not for covid-related tests or jabs, though, but breast cancer ‘vision’ computer ‘modelling’ and surveillance (not the screening itself it seems). This opens up another whole can of worms:
So what?
To summarise, on 12 Nov 2021, the Ministry of Health established a Panel to be led by Sir Ashley Bloomfield who were to meet regularly, read and consider the applications for those Kiwis who applied for an exemption under the SSD Vaccination Order ‘emergency’ laws. Of the 11,741 individuals listed in the applications made, only 68% (8,051) were granted. And of those granted, most, 5,217(ish) were from District Health Boards (more on that soon). All 49 of the applications from Allied Health were declined. But a staggering 2,467 of those granted were not from other patient-serving, under-staffed, poorly-funded public sectors, but instead from corporate giant NZ Health Group.
Remember this was never about Public Health!
Jane Kelley was employed as a Senior Director for the NZ Government’s ‘Covid 19 Response’ by the Ministry of Health in or around Jan 2020. According to her Linkedin profile, she was undertaking ‘consultancy’ work (for Government) between Aug 2021 until Nov 2023 at which point she was appointed CEO of the NZ Health Group. This is the same company which inexplicably benefited from nearly a third of all ‘vaccine’ mandate exemptions, which allowed private healthcare provision to continue throughout the totalitarian era, inevitably pushing up profits for its wealthy shareholders with their private jets. I can’t help wondering what Kelley’s consultancy fees are, and her new salary (although there are some useful clues).
Worldwide, ethical lawyers are working hard to reclaim our Human Rights, that were lost during the covid era. There has been some wins like the NZ Police and Defence Force. But progress is slow.
Finally, it’s worth noting this excerpt from the Healthcare NZ Bio about the wealthy main NZ Health Group Shareholder, Catley:
In the past, Doug has been the Deputy plus Acting Chairman of the Wellington Area Health Board and Chairman of its Policy and Finance Committee. He has also been a member of the Council for the University of Otago’s Wellington School of Medicine, a member of the Medical Research Foundation, and Deputy Chairman of the Board for a major New Zealand bank (TrustBank), the latter being a Prime Ministerial appointment.
(It’s not what you know…)
Meanwhile, our qualified, loyal and experienced public sector workers, including desperately needed nurses, were unfairly discriminated against and declined access to even apply for an exemption, let alone be granted one. Like many of us, they are still being discriminated against today, as I explain here.
If you have further information about this topic, please comment or message me privately. The PDF of the OIA’s spreadsheet should appear below:
It is tempting to think of evil in apocalyptic imagery: vast and sudden demolition, a searing propulsive darkness or a blinding conflagration, the work of engineered catastrophic mayhem, in whose wake is utter smouldering demise. Yet the work of evil is often piecemeal, steady, methodical, and the accomplishment of a great wrong may well be the result of the gradual accumulative weight of small decisions, whose progress is all the surer for its studied implacability. I think of a large battalion of infantry moving painstakingly across a terrain and claiming it inch by inch until they have vanquished all. Yet, in truth, evil is varied, its manifestations as many as there are living human entities who, faced with seemingly slight or casual choices, often land on the side of self-interest, self-aggrandizement and deception. And evil, however disguised, appears in language.
NewZealandDoc’s Newsletter is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
You will forgive me this preface as I alight on a matter that demonstrates with simple clarity a facet of the evil that has been visited upon us during the Corona War by an institution purporting to have as its charge the protection of the public weal in its regulation of medical practitioners: the infamous Medical Council of New Zealand.
On 5 December 2019, while in the employ as a psychiatrist of one of New Zealand’s District Health Boards (since amalgamated into an overarching bureaucratic entity now known as Te Whatu Ora), I received an email communication about informed consent. The document can be perused in its entirety here:
The “Updated statement on informed consent,” signed by Chief Executive Officer Joan Simeon –now, coincidentally enough, the Chair of the Federation of State Medical Board’s international arm, the International Association of Medical Regulatory Agencies – states the following:
“The key points about informed consent are:
•Every time treatment is provided, a doctor must have permission to provide that treatment. The process of obtaining that permission is called ‘informed consent’. Without informed consent, the treatment may be unlawful. To help the patient decide whether they want a treatment, they first need to be given information, such as the risks and benefits of their treatment options.
•Obtaining consent is a process of shared decision-making where a doctor helps the patient understand their medical condition and the options for treating (or not treating) that condition. It is more than signing forms and completing paperwork. As a doctor, you need to take the time to ask questions so that you understand what matters to your patient, and what their concerns, wishes, goals and values are.”
Bear in mind that this statement, meant to be a standard of good medical practice and to be used as a measure of professional conduct, appeared just as covid had been unleashed upon the world.
Then, on 28 April 2021, this very same Medical Council, in conjunction with the Dental Council, issued a guidance statement on professional responsibility and the Covid-19 vaccine (so-called), which can be found here. It was withdrawn without fanfare on 13 September 2023. It is a masterpiece of obfuscation and an inversion of true informed consent. As such, it represents one of those unheralded but highly effective acts of evil.
Guidance Statement Covid 19 Vaccine And Your Professional Responsibility
Not only are health practitioners themselves expected to get the jab, but the regulators write that “it is our view that there is no place for anti-vaccination messages in professional health practice, nor any promotion of antivaccination claims including on social media and advertising by health practitioners,” while simultaneously advising that “As a health practitioner, you have a role in providing evidence-based advice and information about the COVID-19 vaccination to others. You should be prepared to discuss evidence-based information about vaccination and its benefits to assist informed decision making.”
Yet when one of my colleagues undertook to provide advice to a pregnant woman about medical issues connected with the use of the Pfizer inoculation, his licence was suspended. Furthermore, given the provisional approval of the inoculation at the time and the absence of long-term safety data, the much-vaunted informed consent process and the collaborative partnership with patients implied necessitated a frank discussion of serious risk – risk that has, sadly enough, been borne out not only in New Zealand but world-wide, with an extraordinary panoply of adverse events, including death, amounting to a genocide.
With every day each of us is confronted by choice, on matters small or large. However mauled we may or may not be by spike proteins, jabs, hippocampal lesions, or the weight of the massive psychological operation played against us with covid, we retain the freedom to choose. During the Holocaust perpetrated by Nazi Germany – in an era far before viral or vaccine-mediated bioweapons were in play – ordinary people made choices, bureaucrats made choices, neighbors made choices, and a tremendous evil was allowed to grow to a horrific immensity.
Undermining a real, a true, a genuine foundational principle of Medicine – informed consent – in the service of … of following an agenda that has oppressed and is still oppressing us and destroying viable and decent Medicine in the process, is but another one of those examples of how evil wins its way in our world. The Medical Council of New Zealand, ostensible protector of public health, has in its serpentine and devious manner, shown us that it is as destructive as it is hypocritical, and as corrupt as it is authoritarian.
And those many doctors out there who knew then and now know even better about their profession need to come out of hiding, no matter how uneasy or fearful of the “authorities” they may feel.
Unless they do so a medical profession worth keeping won’t be left.
Dan Picknell, also blowing the whistle, was previously interviewed by Liz Gunn at FreeNZ. Hear him at this link
Dan talks here in this interview with Barry Young … hear their thoughts on this entire scenario. The shocking data that the NZ Govt is continuing to debunk whilst promoting still the notorious ‘safe & effective’.
A point to note, Dan speaks early in the interview about how the Police force has changed. This resonates with revelations from another former Snr Detective who communicated with me a few years back. You can read about that here and here.
Even if you believed the debunkers, there is still enough evidence in the data to call a halt and investigate… instead the NZ corporation is continuing to claim ‘safe & effective’... EWNZ
I will debunk these as needed. I’m also offering to bet $250K or more that the NZ data can be used with publicly available data to show that the COVID vaccines are killing people. Any takers??
Executive summary
A bunch of people are making attempts to discredit the NZ data leaked by Barry Young who is now facing 7 years in prison for his actions.
All of the “analyses” claiming “there is nothing to see here” are flawed, but I’ll let you decide that for yourself.
I assure you the NZ data is real and all attempts to discredit the data and what it says will backfire on those who attempt to do so as I will demonstrate in this post.
I’m offering to bet anyone $250K or more that the NZ data shows the vaccines are unsafe. I’ll be thrilled if I get any takers.
But this shows you that none of the people who boldly claim I got it wrong have any confidence in their “analyses.”
CLAIM: “The “New-Zealand whistle-blower” story is a dead-end for valid arguments”
“Too many people are falling for the New Zealand Data trap. There are no alert signal (sic) in the New Zealand mortality trends and the data released is unusable.”
“Alterations made to the data by Kirsch are forbidding serious re-analysis”
“The data made public has been “obfuscated”. In layman terms, this means it has become impossible to verify, and useless for any form of real analysis”
For all 8 ten year age groups listed in the article, 20 and older, as well as for all age groups combined, the per capita deaths in 2022 were higher than 2020.
“Furthermore, Kirsch is now undermining Andrew Bridgen’s efforts in the United Kingdom”
Wow. This is an evidence free post. Let me respond to each point.
There are huge alert signals if you have spent time with the data. The definitive analysis method for an intervention like this is the time-series cohort analysis. Yet OpenVAET doesn’t even mention they looked at it. That’s just ridiculous. He simply does a population analysis and finds that deaths are up for all 8 ten year age groups compared to 2020, so he says nothing is happening in New Zealand. Here is the mortality by week in New Zealand. Does it look like nothing is happening here?
If the vaccines are so safe, why was there a huge mortality peak during the week of July 18, 2022? It’s still a peak even after you remove the COVID deaths. Hmmm…. I wonder why? Also, everyone is vaccinated by then too.
He doesn’t explain what alterations we made, so how can he know the data is unusable? We ran the time series analysis on the original data and on the obfuscated data and the results were an EXACT match. And that’s the definitive way to analyze this data. So I’d like to see his EVIDENCE that the data is unusable for analysis. He provides NONE whatsoever.
See #2.
The data he shows shows mortality increased in every 10 year age group from 20 years on up. So how is that a nothing burger? Had they looked at the time series cohort analysis they would have found huge signals, but they decided not to look.
For proof of #5, they cite this tweet with 153K views. This was Andrew’s idea. Read the comments. Does this sound like I’m undermining his efforts? I was a major funder of the whole event in Parliament.
If you are going to criticize someone’s work, the least you can do is look at it first. If you look at the graph I posted above which is publicly available data (if you know where to look), it’s pretty clear something is wrong and it is crystal clear in the time series data which they NEVER looked at. Something is causing record level peaks.
Claim: “The New Zealand “whistleblower” data is a burger of nothing.”
This new article is co-authored by Dr. Ah Khan Syed.
The key claims include:
This is the definitive takedown. There is nothing to see here. The debate is over.
“The rise in mortality in NZ appears to be explained by the increase in the elderly component of the overall population. That in itself is somewhat bizarre but not a subject for today’s analysis.”
“This curve shows nothing but a slight increase explained by the aging of the cohort.”
What you can see is that there are actually less deaths in the cohort than should be expected based on the background data – about 14% less
The data was deliberately “released as bait” and it under-reports deaths:
Wow. Once again, they ignore the accepted definitive way to analyze the data (time series cohort analysis) and they “roll their own” analysis method and model. They cannot be questioned on this since they are the experts and they don’t have real names. So let’s tackle their key points:
Anyone who claims their analysis is the final word shouldn’t be trusted. Science is all about questioning and being open to be questioned. These “scientists” are claiming they got it right and the case is closed. The NZ data has lots of signals. Just because these two people are incapable of finding the signal is not proof that the signal isn’t there. And the fact that they never look at the time series data and claim no signal is preposterous. They’ve both destroyed their credibility here. In the earlier article, they said that the data can’t be used for analysis. Now they say that they’ve analyzed that same data and there’s nothing to see there. Which is it? You cannot have it both ways.
Wow. Maybe you should get to the bottom of the mortality rise issue before declaring the data Barry released don’t show anything?
The curve they show is too confounded to show anything. And then they give a hand-waving “This curve shows nothing but a slight increase explained by the aging of the cohort.” Really? Where is the evidence behind that statement?
There are less deaths in the cohorts when they first get the shot. It’s called HVE and there are two types. I talk extensively about this in my upcoming article on the NZ data. They are completely unaware of the effect which tells you that they are newbies with respect to analyzing vaccine safety data.
Where is the evidence this was “bait?” AFAIK, there has NEVER in human history been a case where a health authority released manipulated data in the guise of a data breach. Any health authority that pulled such a stunt would destroy any remaining credibility that they had. The authors do not cite a precedent. I’ve spent hours talking to Barry and nearly 2 months analyzing the data and I am constantly amazed how it passes all the statistical “tests” I throw at it. I analyzed it in ways nobody would have thought of and the data is well behaved with no anomalies. If the data is bait, where is the proof in the data or in an admission? These people are simply making this stuff up out of thin air.
Igor Chudov’s analysis
Igor had the good sense to re-think his earlier comments. See this post.
The Barry Young analysis by lot number and the M.O.A.R. analysis
I have been focused on the big picture (the time series cohort analysis).
I have not had a chance to look at the lot number analysis in detail. There are 124 lots to look at.
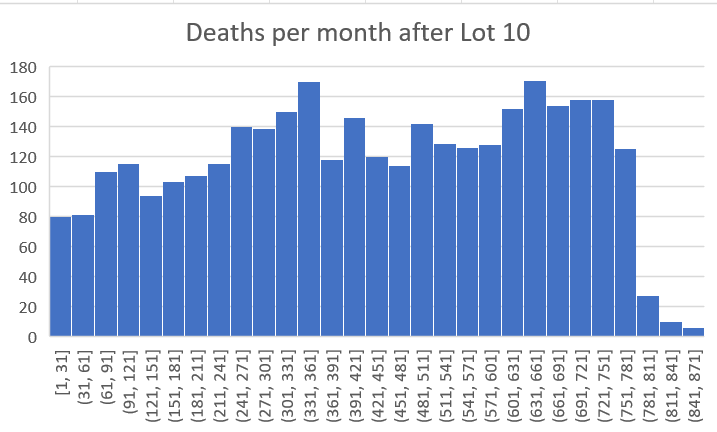
Here’s an example of a huge safety signal in Lot #10:
Deaths per month after Dose 10. This can’t happen for a safe vaccine. Do you know why?
This pattern is impossible for a safe vaccine.
Yet none of the “experts” will be able to tell you why! I’ll reveal why in my upcoming article. Everyone who claims to be able to analyze data should be talking about this!
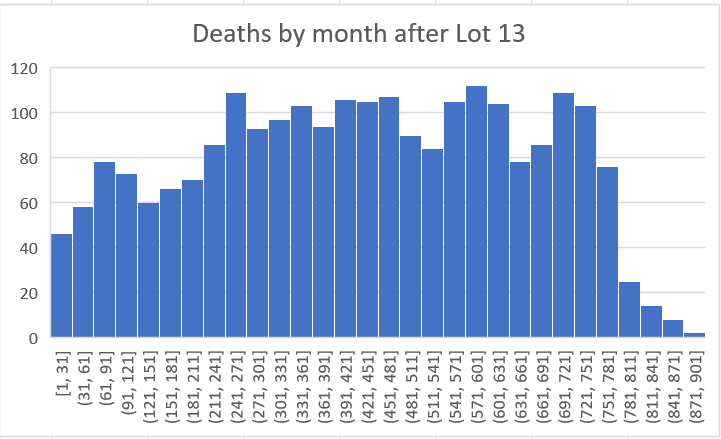
Here’s another example to show this wasn’t a fluke:
Here’s another example to show that Lot 10 wasn’t a fluke
And here’s a third example that is even more stunning than the previous 2 charts:
Here’s another example
Again, the “experts” have absolutely no clue why these charts are so stunning. That’s one of many reasons they say this data is a nothing burger.
What they are really saying to you is “I don’t know how to analyze this data, but I’m going to attempt to convince you that I know what I’m doing and that Steve Kirsch doesn’t.”
History has shown that is a losing proposition.
But just to make this crystal clear to everyone….
My offer to anyone who think there is not a serious safety signal in the leaked NZ data or that the data was gamed or unusable
I’m willing to bet $250K or more that the data is legit and shows a serious safety signal. Anyone want to take my bet? Same terms as my bet with Saar Wilf (neutral panel of expert epidemiologist judges picked by a mutually agreeable consulting firm who vote secretly).
I set the bar at $250K but I’m willing to go to $10M on this one.
I predict crickets.
People who claim I’m wrong and who won’t accept my bet are basically telling you that they have no confidence whatsoever in their analysis.
In Texas, they have a saying for that: “Big hat, no cattle.”
Money is a great way to make that clear to people.
What do you think?
POLL
Do you think anyone will take my $250K or more bet?
Yes
No
1039 VOTES · 6 DAYS REMAINING (visit the link to vote)
Summary
I will update this article as more “analyses” come out.
My advice in the meantime:
If they aren’t doing a careful analysis of the time series cohort data, stop reading.
If they claim the data shows the vaccine is safe or is reducing all-cause mortality, stop reading.
If they claim that the data is insufficient, missing data, systematically biased in a way that makes it unusable, manipulated, false, or that you need a control comparison group (i.e., data that is not publicly available), stop reading.
If they aren’t accepting my $250K or more bet, they are basically telling you they aren’t really sure whether they got it right or not. Otherwise, why not take my money?
I’ll be coming out with my own extensive analysis of the NZ data shortly which will make all these points crystal clear. In the meantime, the lack of any takers of my offer should be a pretty good clue as to who got it right.
As my friend Robert “St. Augustine” Malone has wisely said, “Truth is like a lion: Let it loose and it will defend itself.” The truth has now been set free. Why aren’t you showing us your analysis?
Heath New Zealand’s attitude about public health data reminds me of this classic scene from the Treasure of the Sierra Madre. Click the image to watch the clip. It is hilarious.
When Health New Zealand’s (HNZ) Oracle DB administrator, Barry Young, sent the entire leadership team of HNZ an email to notify them of a huge safety signal in their own database, they didn’t ask any questions: they fired him immediately.
So Barry released the anonymized data which would expose the truth about what the New Zealand public health records contain without violating anyone’s privacy. 4M of the 12M records.
HNZ then decided to try to stop the truth from getting out. So they contacted Wasabi and MEGA and had them nuke my account and Kevin McKernan’s account even though neither of us had done anything wrong. Kevin lost years of work that cost him hundreds of thousands of dollars to create. This is work relied on by other researchers all over the world.
HNZ failed to stop the distribution of the truth. EPIC FAIL.
So now what?
The genie is now (finally) out of the bottle, thanks to HNZ employee Barry Young
Barry will likely spend 7 years in prison for the crime of exposing a crime.
HNZ: I have an important message for you.
The only way you can mitigate damages now is to show us your analysis of your own data showing the COVID vaccines are completely safe.
Why are you hiding this? Surely, you have the analysis. Show us all the analyses you did since the start of the vaccine rollout. You have to show us all documents with dates, showing us every safety analysis you did on your own data. If you don’t we’ll get it via FOIA request.
It would be a more efficient use of your time to simply publish all these analyses now, rather than have hundreds of New Zealanders request it.
The only thing you can be sure of is that not a single mainstream media organization in the world will ask you for these analyses. Like you, they want to keep it hidden. So the NZ press, the New York Times, Wall St. Journal, CNN, 60 Minutes… you’re safe from them. They are never going to ask questions. The vaccine will never be unsafe in their eyes. They are all paid to look the other way by their advertisers.
But the public will ask via FOIA and you’ll have to respond. Are you going to fabricate documents that never existed? That would be criminal.
Or are you going to admit you never did a proper analysis of the data just like the California Department of Public Health never bothered to do any analysis either. Admit the truth.
Bottom line: Show us your analysis now, or the people of New Zealand will require it be produced under FOIA.
HNZ: Where am I? Kirsch (not identified as yet): In New Zealand. HNZ: What do you want? Kirsch: Information. HNZ: Whose side are you on? Kirsch: We are on the side of truth and transparency. We want information…information… information!!! HNZ: You won’t get it! Kirsch: By hook or by crook, we will. HNZ: Who are you? Kirsch: I am the world’s most dangerous misinformation superspreader. Type that phrase into Google; I’m the top hit!! I am your worst enemy. The reason I am so dangerous is that I have been calling for data transparency of public health information (that, by the way, is owned by the public). The medical community, health authorities, and mainstream media all seem intent in hiding the truth. They will lose. The truth always wins. Did you know that the people who try to suppress the truth and achieve medical consensus by means of intimidation, censorship, and coercion are always on the wrong side of the issue? There are no counterexamples in history. Think about it.
Why can’t we talk about it? Let’s have a civil scientific dialog, shall we?
How about we have a publicly recorded video call with your epidemiologists vs. my epidemiologists so we can expose who is telling the truth and who is killing people? Since you can’t stop the distribution of the public health data, this is your only option if you want to reduce “vaccine hesitancy.”
Thank you for your attention.
And one more thing…
The first rule of holes: when you find yourself in one, stop digging.
Maybe you want to consider withdrawing your criminal charges against Barry Young? He did not commit a crime. He relied on the advice of experts including UK Professor Norman Fenton before releasing the data. Of course, you wouldn’t know that because you never asked him. You never even talked to him before having him arrested. Your actions are despicable.
Have a nice day. And thank you for allowing the data to be set free and drawing world attention to the importance of data transparency. And encouraging other health authorities to do the same!
It’s finally here: record-level data showing vaccine timing and death date. There is no confusion any longer: the vaccines are unsafe and have killed, on average, around 1 person per 1,000 doses.
Executive summary
Today you will get to see the data that nobody wants you to see. FINALLY.
No State or country has ever released record-level public health data on any vaccine.
Privacy is not the reason for this; the data can be easily obfuscated (which we did on this data) so that no record entry would match that of any person, living or dead.
The reason the data is kept secret is simple: it would expose the fact that the COVID vaccines are unsafe, as well as all the vaccines that I have been able to get record-level data on.
Today, thanks to a courageous whistleblower who works at the New Zealand Ministry of Health, we have record-level information from a large population of all ages and are making it public for the first time in history.
There was a YouTube link as well, but YouTube censored it within minutes of posting, just like we knew they would.
Just as you suspected, the COVID vaccines have killed millions of people worldwide, an estimated 1 death per 1,000 doses on average in a standard population.
And now we have the data to prove it.
The MIT slide presentation
You can read my “Is it safe?” MIT presentation slides here. I highly recommend reading the slides and/or watching the livestream. I tried to make the slides self-standing, but the livestream can be helpful in explaining some of the slides.
The presentation has everything you need including the credentials to download all the data (search for “Wasabi” in the PDF version of the slide deck).
Here are the Wasabi credentials to make it easy:
Public API keys: access-key= BDBT2BD1KKIXKPWY3030 secret-key= 5GQVqz9uDsmrYjLuNW24tRPzwPuPe0TTleUdpSF3
You can only access the data-transparency bucket for now. Trust me, there’s more that I’m not disclosing yet (including a new US source other than Medicare).
Wasabi explorer downloads are here for PC and Mac. You can also use CyberDuck or any other S3-compatible browser. Make sure your destination folder is writable when you copy files from the server.
You can also use rclone to make a local copy of the repository on your system:
The data: All the data in the data-transparency bucket is sanitized. Any matches to actual records is completely accidental. The data was sanitized in a way that preserves the statistics. We ran the bucket analysis on the original and obfuscated data and got nearly identical results. There is no reason any health authority couldn’t do the same thing we did.
The tools: We’ll give you our time-series cohort analysis software. This is the software that you’ll never get your State epidemiologist to use. Now, armed with record-level data, you can do your own analysis. We’ve made it super easy to use. When done, paste the output file into our v4 analysis .xlsx spreadsheet and you’ll see instantly whether the vaccine is safe or not.
The analysis documents: You’ll find annotated spreadsheets as well as word documents.
The description of the data: You’ll find documents describing the dataset (size, dates, average ages in each cohort, what the authorities claim, etc.
I encourage you to explore. Everything is “legal” in that jurisdiction. So you’ll see the full times of people who died in the Maldives, for example. In other places, the names are omitted.
Introduction
I was provided the data on November 8, 2023 when it was uploaded to my Wasabi file server.
I was asked by the whistleblower to keep the data confidential until November 30 in order to give the whistleblower time to work out the logistics of how the data would be made public.
I honored my commitment and only shared it with a handful of colleagues including Norman Fenton and his associates in the UK with the whistleblower’s consent.
The data from New Zealand is not perfect; it is not a complete sample. For example, for some people, the first record in the database is Dose #3. Also, only vaccinated people are in the database.
But, by using a cohort time-series analysis, it doesn’t matter. There is no possible way that this data is consistent with a safe vaccine. I estimated that the vaccine killed, on average, about 1 person per 1,000 doses. That means an estimated 675,000 Americans were killed by the COVID vaccines.
We have confirmation of the analysis from the US Medicare data thanks to another whistleblower.
The story of the data can be found in my presentation which has a link to the Wasabi server and access credentials, as well as how to download the free Wasabi File Explorers for PC and Mac. There is a large amount of data and analysis uploaded to the servers.
The cohort time-series analysis takes about 2 hours to run on the data. We’ve included the output files so you can start from that.
Analyzing the data takes about 5 minutes using the v4 spreadsheet in the analysis directory. Anyone can do it. You just plug in numbers to vary the parameters to look at anything you want to investigate. It has 8 visualizations: 4 main graphs (one for each independent variable) and 4 below each graph showing the number of deaths so you can use that to judge the reliability of the data points in the graph above.
Be sure to read the entire presentation to understand how to interpret the data.
Papers about the data
Papers will be coming out from various authors over the coming weeks. See this article which I will update over time.
Summary of what we found
Record level vaccination-date/death data obtained from a whistleblower in the New Zealand Ministry of Health was analyzed using a standard time-series cohort analysis. The results remained consistent even after varying all four of the key independent variables (observation time window, days after shot, age, and dose number). The only way that can happen is if the COVID vaccines significantly increased mortality for those aged 60 and older, the very population that the vaccine was supposed to help. All five Bradford Hill causality criteria are satisfied. From this data, we can accurately estimate that overall, the mRNA vaccines led to the premature death of more than 1 person per 1,000 doses on average over all doses.
This estimate is supported by COVID death data from Medicare obtained from another whistleblower. The data from Medicare was stunning: the number of people who died rose monotonically for those who got shot in 2021 or 2022. My whistleblower inside HHS had never seen anything like that before. It was a perfectly straight line sloping upwards for 365 days since the dose was given. A safe vaccine would see a decline in deaths by 4% to 5% after 1 year from the shot. The COVID vaccines had a 26% mortality increase, a net difference of 30%. This makes the COVID vaccine a competitor to heart disease as the leading cause of death among the elderly (which kills 20% of people per year).
The COVID vaccines are the deadliest vaccine of all time, killing an estimated 13 million people worldwide.
The precautionary principle of medicine requires that a vaccine which results in such a large net increase in all-cause mortality should be immediately revoked worldwide unless there is a more likely explanation for this “gold-standard” data. Nobody has come forward with a better explanation that fits all the data. In fact, nobody on the other side even wants to see this data: the FDA, CDC, Moderna, and Pfizer all refused to look at it. How is that responsible? That is reprehensible.
Researchers could have discovered the harms of these vaccines years earlier if any of the world’s health authorities released comparable record-level data to that released here. It is baffling to us why the medical community who is sworn to do no harm is not insisting on seeing any record-level data before recommending the use of any vaccine to their patients. It is the record-level data that is key to understanding whether a vaccine is safe or not. This is always hidden from public view.
Hidden from view?!?!
Clinical outcomes are never improved by keeping public health data hidden from public view. Yet every health authority in the world has kept this critical record-level safety data hidden from view.
And, to our knowledge, only one authority, the UK Office of National Statistics, had supplied even the most basic time-series analysis for a limited amount of time. The UK time-series analysis confirms the monotonic increase in mortality after each shot is given. But the UK ONS got to pick the bucket sizes whereas when we do the analysis, we have buckets for every week so we can see exactly what is going on. They can’t. And the ONS stopped responding to me when I asked to see the record-level data.
Other health authorities apparently refused to analyze their own data themselves to look for any safety signals which we found in abundance just minutes after receiving the data. After we received this data and analyzed this, we reached out to a number of health authorities in the US in Florida, California, and at the CDC and FDA. They all ignored the request to examine the data I obtained or look at their own data. This is the first time in history that vaccination-death record-level data has been made available to the public. And now we know why.
In addition, FOIA requests to the California Department of Public Health showed that they never analyzed their own data. There were no documents showing that they ever looked for any safety signals. They simply trusted the CDC even though the CDC doesn’t have any vaccine record level data, so it is IMPOSSIBLE for the CDC to do the proper safety analysis.
Finally, the safety signals are limited to those 60 and over simply because there wasn’t enough data to make a firm determination for people under 60; the data was simply too noisy because we were only given 4M of the 12M records in New Zealand.
However, since the vaccine provides no benefits whatsoever for infection, hospitalization, or death, there is no reason for anyone in the world to take these vaccines. See the presentation for details.
In any sane world, the COVID vaccines would be immediately halted and inquiries should begin as to why no health authority in the world did a thorough cohort time-series analysis on the data which would have uncovered the safety signal very early in the deployment. Are they all corrupt? Or are they all incompetent? Or both?
Can Moderna survive this? Why would anyone buy their stock?
These results have implications for Moderna stock as the failure of their underlying technology casts serious doubt on their viability as a going concern. Even if governments continue to buy their products, the breach of the public trust and the unwillingness of the company to look at the record-level data shows that the company is more interested in making a profit than ensuring the safety of their customers. A head in the sand approach to safety is despicable.
Pfizer is no different. Both companies were offered an opportunity to view this safety data and they all refused. So did the FDA and CDC. The offer was made by a respected journalist in the medical new community, not by me.
What did Professor Norman Fenton say about this new data?
Nobody should take my word on this. Those are my opinions based on examination of the data.
Anyone can analyze this data. Come to your own conclusions.
Finally, here is what famed British Mathematician Professor Norman Fenton said, “This confirms what we also saw in the most recent ONS data once.
Whatever uncertainty there may be in the younger age groups there is now no doubt the vaccine is increasing the mortality rate in older people.”
I agree. In spades. I’d bet my life on it.
Yale epidemiologist Professor Harvey Risch had this to say:
“I think that you’ve made a very strong case that the Covid genetic vaccines are associated with appreciably increased mortality rates for 6-12 months after each dose. This is particularly compelling in people over age 65. I am not aware of actual evidence that the increased post-vaccine mortality that you’ve shown has a different cause.”
The English translation of what he wrote is “the vaccines are killing people,” but scientists aren’t allowed to be blunt so they have to qualify everything they say.
This is how today’s “scientists” come to conclusions
If there was a mass shooting and everyone died, a scientist would want to have a control group and complete medical histories of each person (including a list of comorbidities) and then want to do a Cox proportional hazards analysis before concluding that the gunman could be the cause of death of these people. Without a control group, the scientist would be unable to say whether the shooting actually caused the deaths.
Nobody with respectable credentials wants to defend the vaccine as being safe
I offered to engage in a public recorded debate with anyone who thinks we got it wrong. Nobody was willing to do that to date, although Professor Jovo Vogelstein offered to give it a try to play devil’s advocate.
If you think we got it wrong, I have a $500K bet pending with Saar Wilf in Israel. I’d love to increase the stakes on that bet. Any takers?
Some people are just never going to figure this out
UPenn Professor Jeffrey Morris has had the data for a while. He doesn’t agree with our analysis (as expected). But when I asked him to explain the Medicare data where the mortality monotonically increases every day for 365 days straight, he said he refused to speculate. Professor Morris never is able to see a vaccine that is unsafe. I proposed all sorts of unsafe hypotheses to him, and he said none of them were convincing. So in his mind, no matter which way the deaths go, even if they go sky high after the vaccine is given, you cannot tell if a vaccine is safe or not; there will always be a confounder that he will find. And he’ll always insist on getting additional data that is never available, so he’ll argue that all data, no matter how strong, is not good enough.
Nearly half of America has already figured out the COVID vaccines are not safe; they want to sue the drug companies!
Some people will try to convince you that the data isn’t complete and is confounded for that reason. That’s bullshit. If it’s a safe vaccine, you can be missing 99% of the shot data and still get the right answer. Doses don’t matter; a safe vaccine is like a saline shot: they cause no impact.
They won’t get away with stupid arguments like that with me. That’s why they won’t debate me.
Consider supporting my work with a paid subscription
I only have time to do this work because this is my day job.
If you liked this article and want to keep supporting my work, and are not already a paid subscriber, please consider becoming a paid subscriber for just $50/yr or $5/month.
Your subscription fee supports the critical work that Substack has done in providing a free-speech platform, and also provides the funds needed to continue this work to expose the fraud and save lives.
Having trouble? Use the Contact me link
You can get support here using the Contact Me link.
Summary
It’s over. They’ve lost. The vaccines are unsafe. This data is the nail in the coffin. Gold standard, official records. There is no better ground truth than this.There is no comparable ground-truth data showing the vaccines are safe. Zero. There can be only one right answer.
If you think the vaccines are safe, accept my bet, debate me publicly, or release the record level data in your state. Nobody will do any of those things it seems.
Sooner or later top epidemiologists will weigh in on this data.
Now we’ll see just how broken science is if the world’s top epidemiologists cannot agree that the vaccines are unsafe. For example, will John Ioannidis weigh in? Or will he remain silent? Will Martin Kulldorff say anything? Or will he also ignore this data?
In the meantime, the medical community and mainstream media will keep recommending the jabs as if nothing has happened. They should be ashamed of themselves.
Remember your government has released Pfizer from any liability for their product if it happens to harm you (and it has, unless you are believing mainstream spin). Listen to this woman whose experience proved you’re on your own if things go wrong. EWR
Posted on NZ MOH site, June 3 2021
Taken from a transcript of a webinar by a MOH Covid Committee, who hold fortnightly webinars for health professionals.
Do health professionals appreciate the implications for this statement made by the facilitator, I wonder?
The facilitator states… ‘There were a couple of questions at the last meeting that came through so I’m just going to run those off quickly. The first was around funding to support primary care when people are presenting to them with side effects following their vaccination. There is no specific funding available to cover that and no specific funding to cover the submission of an adverse event into CARM so there isn’t any funding to cover that. I’m going to touch base, I spoke to the post-event team leader today just to follow up with him and he’s organising for me the contacts at ACC so we can understand what is the threshold at which we can make a claim through ACC that this is a treatment injury. I haven’t seen those yet, but we will follow that up and see where it takes us.’
I would ask, ‘see where it takes us…’ Really?’
After all this time and this is where the MOH is at? So much for robust processes, transparency, safe and effective ‘vaccine,’ post adverse injection event planning? How would the Team of 5 million respond to this absence of due diligence, if this was included in the Government Briefings, I wonder? What can anyone expect, in terms of a duty of care, if one is unfortunate enough to experience an adverse reaction in NZ, to the Pfizer Comirnaty injection? How much money is paid to employ the experts on this panel? No problem finding funds for their salaries?
I would post the link, but it’s gone, along with the complete transcript and additional information. If you request it under the OIA, will you be informed that like most documents so far, this is ‘confidential?’ We seem to have an epidemic of ‘confidentiality’ for those who are employed to ensure Regulation, Assurance and Protection are complied with and no ‘Community Immunity’ for ‘Transparency.’ Maybe someone who is a health professional can access the webinar link? The complete webinar and the section of concern, watch from the 4.12 minute mark. https://youtu.be/hIyyJ6s0oRM
Note: the commentary for this post from fb is author unknown, please advise if you wrote it. I did try to locate the author. EWR











![WHEN EXPOSING A CRIME IS TREATED AS COMMITTING A CRIME, YOU ARE BEING RULED BY CRIMINALS. - Edward Snowden [783 x 391] : r/QuotesPorn](https://substackcdn.com/image/fetch/f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fsubstack-post-media.s3.amazonaws.com%2Fpublic%2Fimages%2Fe23a0c4a-09db-42d3-97f6-70cd6df9fd17_783x391.jpeg "WHEN EXPOSING A CRIME IS TREATED AS COMMITTING A CRIME, YOU ARE BEING RULED BY CRIMINALS. - Edward Snowden [783 x 391] : r/QuotesPorn")





