Dan Picknell, also blowing the whistle, was previously interviewed by Liz Gunn at FreeNZ. Hear him at this link
Dan talks here in this interview with Barry Young … hear their thoughts on this entire scenario. The shocking data that the NZ Govt is continuing to debunk whilst promoting still the notorious ‘safe & effective’.
A point to note, Dan speaks early in the interview about how the Police force has changed. This resonates with revelations from another former Snr Detective who communicated with me a few years back. You can read about that here and here.
Shocking data released by the UK Government shows that over the past two years, the vaccinated population in England have suffered an outrageous number of deaths compared to the unvaccinated population despite the fact approximately 30% of the population has not even had a single dose of the COVID-19 vaccine.
According to the UK Government department known as the UK Health Agency (UKHSA), by 3rd July 2022, 18.9 million people had refused the first dose of the COVID-19 injection, 21.5 million people had refused the 2nd dose of the COVID-19 injection, alongside 2.6 million people who had received the first dose but refused the second, and 30.4 million people had refused the third dose of the Covid-19 injection alongside 8.9 million people who had received the second dose but refused the third. (Source)
According to the UKHSA’s figures, 63.4 million people were eligible for vaccination at this point. Therefore, 18.9 million people refused the COVID-19 vaccine in England and remained completely unvaccinated.
But on top of this, a further 2.6 million refused a second dose, meaning 21.5 million people were not double vaccinated, and 8.9 million people refused a third dose, meaning 30.4 million people were not triple vaccinated.
Here’s how those figures equate in terms of percentages –
In July 2022, thirty per cent of the population of England remained completely unvaccinated. 34% of the population of England were not double vaccinated, and 50% of the population were not triple vaccinated.
However, as is shown in the following chart, the vaccinated population as a whole accounted for 95% of all COVID-19 deaths between January and May 2023, while the unvaccinated population accounted for just 5%.
But it’s the fact that these deaths aren’t among the one-dose and two-dose vaccinated population that is truly horrifying. The vast majority are among the 4x vaccinated, with this population accounting for 80% of all COVID-19 deaths, and 83% of all COVID-19 deaths among the vaccinated. (Source)
So with that being said, the following figures published by the Office for National Statistics (ONS) in their ‘Deaths by Vaccination Status’ dataset, which can be found on the ONS website here, or downloaded here make for even more horrifying reading.
The following graphs show all-cause deaths by vaccination status between July 1st 2021 and May 31st 2023 by age group. Each graph can be expanded by clicking on it to see the figures more clearly. The unvaccinated deaths are shown first in each age group and the vaccinated deaths are shown next in each age group.
But you don’t even need to zoom in to see the horrendous difference in deaths by vaccination status.
Between July and September 2021, the highest number of unvaccinated all-cause deaths occurred among 70 to 79-year-olds in August with 676 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among the 80 to 89-year-olds in September 2021 with a shocking 13,294 deaths.
Between October and December 2021, the highest number of unvaccinated all-cause deaths occurred among 80 to 89-year-olds in December with 776 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among the 80 to 89-year-olds in December 2021 with a shocking 16,171 deaths.
Between January and March 2022, the highest number of unvaccinated all-cause deaths occurred among 70 to 79-year-olds in January with 776 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among the 80 to 89-year-olds in January 2022 with a shocking 15,948 deaths.
Between April and June 2022, the highest number of unvaccinated all-cause deaths occurred among 80 to 89-year-olds in April with 500 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among the 80 to 89-year-olds in April 2022 with a shocking 14,902 deaths.
Between July and September 2022, the highest number of unvaccinated all-cause deaths occurred among 80 to 89-year-olds in July with 493 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among the 80 to 89-year-olds in July 2022 with a shocking 14,286 deaths.
Between October and December 2022, the highest number of unvaccinated all-cause deaths occurred among 80 to 89-year-olds in December with 604 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among the 80 to 89-year-olds in December 2022 with a shocking 19,914 deaths.
Between January and March 2023, the highest number of unvaccinated all-cause deaths occurred among 80 to 89-year-olds in January 2023 with 551 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among the 80 to 89-year-olds in January 2023 with a shocking 18,297 deaths.
Between April and May 2023, the highest number of unvaccinated all-cause deaths occurred among 70 to 79-year-olds in May 2023 with 405 deaths. Whereas the highest number of vaccinated all-cause deaths occurred among 80 to 89-year-olds in April 2023 with a shocking 13,713 deaths.
What’s extremely concerning about these official figures is that the vaccinated surpass the unvaccinated by far in terms of death in every single age group since July 2021, despite the fact 30% of the population have not even had a COVID-19 injection.
So much so, that there were 965,609 deaths among the vaccinated compared to just 60,903 deaths among the unvaccinated between July 2021 and May 2023. Meaning there was a grand total of 1,026,512 deaths in England during this period and the vaccinated accounted for 94% of them, whereas the unvaccinated accounted for just 6% of them.
This more suggests that the Covid-19 injections are deadly, and prove that they are killing people. And we can be certain that COVID-19 Vaccination greatly increases mortality.
So when will the Government discontinue their use?
The World Health Organization’s pandemic treaty, the amendments to the International Health Regulations (IHRs) and the global One Health agenda are all part of a soft coup, a global power grab
The globalists’ plan for our future can be summarized as “global dominion by the few and total control of the masses”
The technocratic cabal has control over most if not all Western governments, as well as the bureaucratic structure of the WHO; 85% of its funding comes from private entities, so it’s owned by private interests
Based on the current treaty draft and proposed IHR amendments, it’s clear that mRNA-based vaccinations will be mandatory under the WHO’s power structure, and these vaccines will be made in 100 days by skipping human trials and shaving safety and efficacy testing down to the bare bones
Under the treaty, as currently written, nations will be required to surveil and censor social media. The WHO’s narrative will be the only one allowed
In this September 1, 2023, Highwire interview,1 Dr. Meryl Nass, a biowarfare and epidemics expert, exposes the threat posed by the World Health Organization’s pandemic treaty and the amendments to the International Health Regulations (IHRs), which add to and further strengthen the WHO’s powers under the treaty. The WHO’s One Health agenda is also part of this power grab.
Nass also recently published an article, “The WHO’s Proposed Treaty Will Increase Manmade Pandemics,”2,3 in which she reviews the history of biological warfare and the role of gain-of-function research, where we are right now, and what the globalists’ plan for our future is. It’s imperative everyone understand what the plan is, because we can only stop it by rejecting it en masse.
Nass Persecuted by Lawless State Medical Board
But first, Nass provides an update on her personal situation. In January 2022, the Maine medical board suspended Nass’ medical license for spreading “COVID misinformation” and prescribing ivermectin. They also ordered her to undergo a psychological evaluation by a board-selected psychologist.4 Nass refused.
As she points out in the interview, “misinformation” refers to information that may be mistaken or inaccurate, but being wrong is not a crime — no matter how badly government wants you to think it is.
We have the First Amendment — freedom of speech — for a reason. Government does not have the legal right to suppress our speech, and the medical board is a state government agency. So, by censoring doctors like Nass and punishing them for speaking their minds and sharing medical and scientific data, they are actually the ones breaking the law.
Nass didn’t, because there’s no law against sharing information, even if it is suspected of being incorrect, or can be proven to be wrong. And, in this case, the board is actually punishing her for sharing truths.
So, in mid-August 2023, Nass sued the Maine medical board, and every board member in their personal capacity, for violating her free speech rights.5
“Telling me that I can’t talk about the vaccine or I can’t talk about the treatment of COVID or masks or distancing, even when the things that I was saying were based on published medical literature, that is a First Amendment violation,” Nass said in a statement.
“The state government and the federal government are not allowed to restrict the speech of people. So we are looking for a jury trial to see whether the Board of Licensure in Medicine is guilty of a malicious, political prosecution and targeting of me.”
The Plan in Broad Strokes
So, what is the globalists plan for our future? Summarized into as few words as possible: global dominion by the few and total control of the masses.
As explained by Nass, the COVID pandemic showed us that the technocratic cabal has control over most if not all Western governments. World Economic Forum (WEF) founder Klaus Schwab has even bragged about how his Young Global Leaders have “penetrated” governments of the world.6
The technocratic cabal also has control over the bureaucratic structure of the WHO. Eighty-five percent of the WHO’s funding comes from private entities, most of which is earmarked for specific programs. “So, the WHO is already owned by private interests,” Nass says.
According to the WHO, the reason the COVID pandemic got so bad is because nations failed to cooperate. Hence, the reasoning goes, we need an international treaty that centralizes pandemic response powers to the WHO. The problem, of course, is that most nations did follow the WHO’s irrational and unscientific recommendations. Its ineptitude — whether intentional or not — is what destroyed economies and resulted in needless deaths.
Based on the current treaty draft and proposed IHR amendments, it’s clear that mRNA-based vaccinations will be mandatory under the WHO’s power structure, and these vaccines will be made in 100 days rather than 10 years by skipping human trials and shaving safety and efficacy testing down to the bare bones.
The WHO will also decide which medications can be used in medical emergencies, and which you cannot have. In other words, the WHO director-general will decide the health care for every person in every member state, and your local doctor will be required to follow his edicts. You’ll have no medical freedom or bodily autonomy anymore.
Nations will also be forced to implement massive nationwide biosurveillance programs to identify potential pathogens with pandemic potential. This will include swabbing and testing humans, domesticated animals, farm animals, wildlife, farms, factories, wastewater and more, and the chances of finding a pathogen with pandemic potential if searching for it in every nook and cranny of the world are 100%.
The WHO director-general will then have the sole authority to declare a pandemic, or even potential pandemic, at which point all decision-making powers fall under the WHO. However, there are no standards that must be met before a public health emergency can be declared.
The way these documents are written, the director-general can even act on what amounts to hearsay. He doesn’t have to have proof that a pandemic is imminent or in progress. He can act on suspicion. Even more disturbing, the treaty will be in force all the time, so the director-general doesn’t even need to declare an emergency. He will have the authority to dictate public health even when there’s no pandemic. That’s how far-reaching this treaty is.
Nations will also be required to surveil and censor social media. The WHO’s narrative will be the only one allowed. YouTube has already implemented this policy, even though the treaty is not even in place yet.
The History of Biological Warfare and How We Got Here
Nass also reviews the history of biological weapons and why we’re in a situation now where most of the pandemics that have occurred are basically the result of biological weapons development.
In 1969, President Nixon announced the U.S. would end its offensive biowarfare program. This was a strategic rather than altruistic move, because the U.S. was far ahead of other nations when it came to chemical and nuclear weapons. By banning biological weapons, which are relatively simple and inexpensive to create, the U.S. would gain a strategic advantage on the global stage.
Nixon initiated the first global treaty to prevent the creation and use of biological weapons in 1972. The Biological Weapons Convention took effect three years later, in 1975. However, in 1973, genetic engineering was discovered, which suddenly allowed the U.S. to gain a technological advantage that would allow us to make better and more precise biological weapons.
The problem with the Biological Weapons Convention is that there’s no enforcement. To be effective and verifiable, a nation needs to be able to challenge another nation and have the right to carry out inspections, and add sanctions in cases of noncompliance. But this enforcement method was not included, and the U.S. has blocked all efforts to add enforcement articles to the treaty since 1991. So, as explained by Nass:7
“Under the guise of preparing their defenses against biowarfare and pandemics, nations have conducted ‘dual-use’ (both offensive and defensive) research and development, which has led to the creation of more deadly and more transmissible microorganisms. And employing new verbiage to shield this effort from scrutiny, biological warfare research was named ‘gain-of-function’ research.”
SARS-CoV-2, for example, appears to be the direct result of gain-of-function research. As noted by Nass, it has “unusual homologies (identical short segments of nucleotides) to human tissues and the HIV virus, which may have caused or contributed to the late autoimmune stage of illness, an impaired immune response and ‘long COVID.’”
As such, SARS-CoV-2 is a biological weapon. David Martin, Ph.D., has also done many interviews, speeches and lectures exposing COVID-19 as a biological warfare crime. https://rumble.com/embed/v2oem0q/?pub=4Video Link
Are We Funding Public Health or Bioweapons Development?
As noted in Nass’ article, funding for natural epidemics, such as seasonal influenza, has been lumped together with biodefense funding, which hides the cost of our nation’s bioweapons development, because in reality, “biodefense” is “bioweapons development.”
And, while bioweapons development is dangerous and violates the international treaty, biodefense is useless and a complete waste of money, so it’s a lose-lose proposition for taxpayers.
In March 2023, former CDC director Dr. Robert Redfield testified before Congress stating that gain-of-function research had never, to his knowledge, resulted in a single beneficial drug, vaccine or therapeutic.8
In other words, while they conduct this research under the guise of “defense,” all gain-of-function research is biological weapons research and has no beneficial public health applications.
The pandemic treaty promotes the proliferation of biological weapons, and opens the door wide to biological weapons research and testing. It will take us in the opposite direction of where we need to go to prevent future pandemics.
The WHO treaty makes matters even worse by requiring member nations to look for pathogens with pandemic potential, and when they find them, to share them, and any research done on them, with everyone else.
So, the WHO treaty quite literally promotes the proliferation of biological weapons, and opens the door wide to biological weapons research and testing. This will also remove the ability to cast blame on any particular nation for starting a pandemic (read unleash a biological weapon), as everyone is working with the same pathogens.
The treaty also requires nations to eliminate administrative hurdles to gain-of-function research on pathogens with pandemic potential, when we really need far more stringent regulations on this type of work, if we’re going to engage in it at all.
So, the WHO treaty will move us in the complete opposite direction of where we actually need to go if we want to prevent future pandemics. To prevent them, we need to stop gain-of-function research, because that’s the greatest pandemic threat out there.
Pandemic Preparedness Is a Smokescreen
Similarly, the idea that the world can prepare ahead of time for a global pandemic is “a smokescreen behind which lies a fascist approach to social management,” Nass writes. She adds:9
“There’s no known way to prevent pandemics, and the methods that governments are spending money on are actually going to make this problem a great deal worse.
The concept of a ‘response’: withholding cheap, available generic drugs in favor of the warp speed development of patentable drugs and vaccines, which will undergo minimal testing and have no liability, is another disaster in the making.”
Our Health Agencies Are Selling Us Out
Importantly, the U.S. government — including our health agencies — have been central in developing and writing these documents, which strips us of our sovereignty as a nation, bodily autonomy as a people, along with freedom, human rights and democracy in general.
Indeed, the IHR amendments specifically remove the need to respect “human rights, dignity and freedom of persons” during public health emergencies. This deletion did not go unnoticed, however, and after severe criticism, language “guaranteeing” human rights was inserted into the latest draft (the Bureau draft) of the pandemic treaty.
The bottom line is, our health agencies are not protecting us. They’re controlled by private, globalist interests, and they’re selling us out.
We also see this in the way the U.S. health agencies like the Centers for Disease Control and Prevention and Food and Drug Administration refused to course correct once it became clear that the COVID shots were not preventing infection or transmission, and were causing historically high rates of injuries.
Instead, they doubled down and imposed mandates, and started fiddling with database algorithms to hide the extent of injuries and deaths. Likewise, the WHO is working on an international vaccine passport, even though the entire premise for it has been eliminated. If the shots don’t prevent infection or transmission, then what good does proof of “vaccination” do?
Same with the masks. No matter how much scientific evidence was thrown at them, health authorities refused to admit that masks don’t work and pushed for wearing two or three masks instead. And what can we say about the worldwide recommendation to treat only advanced-stage infection? It’s medicine 101 to treat a condition as early as possible, especially when it comes to infections.
As noted by Nass, “There can be no question about it: Our health agencies are guilty of malfeasance, misrepresentation and deliberate infliction of harm on their own populations.”
All the basic rules of medicine were tossed out during COVID, and under the pandemic treaty, common sense and basic medical facts will be ousted forever. Nass goes through much more in her article, so I urge you to read it10 in its entirety.
The Timeline
The IHR amendments will only require a 50% vote of whoever is in the room at the time of the vote, which will take place at the World Health Assembly’s annual meeting, May 22 through 24, 2024.11 The amendments will take effect 10 months later for any nation that does not opt out.
Nations that have not officially opted out will then be bound by the new terms laid out in the amendments. The pandemic treaty will also be voted on during that meeting. It will require two-thirds vote in favor by the members that are in the room and will go into effect as soon as 30 nations have ratified it.
Thirty days after that, the treaty will go into effect for all the nations that have signed on. Any nation that has not signed the treaty will be excluded from its terms. Those who sign the treaty must wait three years before they can get out.
Door To Freedom
To prevent this nightmare, Nass has founded a new organization called Door To Freedom (doortofreedom.org), which seeks to educate people around the world about what the pandemic treaty and IHR amendments will change life as we know it, and strip us of every vestige of freedom.
Door To Freedom has created a poster to explain the impacts the pandemic treaty and IHR amendments will have. Please download this poster and share it with everyone you know. Also put it up on public billboards and places where communities share information.
Other Action Items
While the situation seems incredibly bleak, Nass insists there are many things we can do to prevent the WHO’s power grab, including the following:
• Call your congressman or congresswoman and urge them to sponsor H.R.79 — The WHO Withdrawal Act,12 introduced by Rep. Andy Biggs, which calls for defunding and exiting the WHO. At the time of this writing, it has 51 cosponsors, all of them Republicans. We cannot get this bill passed without Democrats, so we need to get them to understand what’s at stake.
The Sovereignty Coalition is making it easier for everyone to make their voices heard. Its Help the House Defund the WHO page will allow you to contact all of your elected representatives with just a few clicks. Simply fill out the required field, click submit, and your contact information will be used to match you with your elected representatives.
• Also urge your congressman or congresswoman to sponsor H.R.1425,13 which would require the pandemic treaty to be approved by the Senate. It currently has 27 cosponsors.
• Share Door To Freedom’s educational poster15 everywhere you can, and direct them to doortofreedom.org for more information. Also share, share, share information about the IHR amendments and how they will destroy national sovereignty, and increase surveillance and censorship. You can find a quick summary here.
We all have friends and family who still believe their Government is benevolent, who think their response to the pandemic has been marvellous, and the mRNA jab is safe and effective. But, of course, the opposite is the reality: Our Government has declared war on its people. They are working for insane foreigner technocrats, who intend to turn us into a totalitarian state, the vaccine is neither safe nor effective, and they are doing everything they can to hide the extent and gravity of their crimes.
Despite the obvious, in-your-face lying about these crimes, for most people, including myself, comprehending the reality and gravity of the situation is far from easy. But unfortunately, continuing to believe monumental lies is the easier path to follow for many people. They may argue that they are too busy, that they already have too much on their plates to deal with. We are told by the Government and their advisers, like the Pink Lady, who is our expert about everything, that they know better than you or anyone else about what is going on, and to such as extent that they’ll fire and publicly ridicule anyone who questions their truths.
One response is to ask them to do just one thing for you and set aside a little time to plug in their headphones and listen to two podcast-style presentations. After that, you can then have a civil discussion about the issues and agree or disagree but continue to be good friends no matter the outcome.
There are many possible presentations to recommend for the busy person, but here are two which should do the job:
(Unlike other broadcasters like Michael Laws and Sean Plunket, Leighton Smith is renowned for meticulously researching his podcast topics and not talking over his guests.)
Leighton Smith Podcast: Statistician and author Guy Hatchard discusses the distortion of public information, and the age of social engineeringLeighton Smith Podcast: Statistician and author Guy Hatchard discuss the distortion of public information and the age of social engineering
I’ll add here that Guy Hatchard and I go back a long time: We were part of a small group of health professionals who have, on two occasions, prevented the passing of the Natural Health Products Bill, which essentially hijacks natural health products, including ones like also vera, vitamin C and zinc to further the aims of Big Pharma and Medical-Industrial Complex. It just happens that the Minister of Health is about to railroad this legislation through the House this year without adequate consultation. If this legislation passes, practitioners like men may become a thing of the past.
”Dr Nikki Turner, you are murdering people! … Now debate me.” – Dr James Thorp MD: This interview, hosted by a couple of Kiwi broadcasters, Kelvyn Alp and Hannah Spierer, now streaming from a USA-based platform, is a beauty. In this interview, an international medical heavyweight calls out New Zealand’s lightweight medical expert for a head-to-head debate.
As an aside, Alp and Spierers’ broadcasting platform was shut down in New Zealand a few months ago, hence the USA presence now. They are currently on bail defending themselves from prosecution by the NZ Government for holding or sharing objectionable information and face what could be years behind bars. if they lose!
Brenton Faithfull is a Funeral Director and a Justice of the Peace. He is well aware of the importance of the truth. Hear his interview with Dr Matt Shelton of the NZ Doctors Speaking Out with Science (NZDSOS).
If you are a double jabbed Kiwi, please read this plea from the heart from your un-jabbed fellow Kiwis. Our nation’s future depends on it.
We are not asking you to agree with us, we are just asking you to hear us and to remember those great Kiwi traits that we have always taken such pride in showing to the rest of the world. Those traits of compassion, empathy, tolerance, and above all, Kiwi unity and courage.
To quote one of the lines from our great national anthem…………“hear our voices we entreat”.
We are all Kiwis and we all love our great country and its people. COVID has been enormously challenging for so many segments of NZ society. So many Kiwis have been so challenged and so hurt through this time, and as a double jabbed Kiwi you are ‘taking one for the team’ to try to help get NZ free and open again. We understand that, and we really respect and admire that sentiment. It is a very Kiwi mentality of rolling the sleeves up, so to speak, and getting on with sorting the problem out.
Note: $130K has been paid out already for covid related claims. The primary headline for the article. However mention is also made of claims related to the jab. Read below:
From newstalkzb
Almost $130,000 has been paid out in Accident Compensation Corporation claims for work-related Covid-19 exposure.
As of August 31, ACC had accepted 13 claims – the majority for healthcare workers – which total $122,974, an average of $9459 per claim.
Claims are identified as related to Covid-19 exposure where the injury description is “coronavirus infection” or the accident description includes either “Covid-19” or “coronavirus”, and “exposure” or “contracted”.
As the accident description is a non-mandatory section of a claim lodgement form, an ACC spokesperson said the data based on this field should be considered indicative only.
ACC has also received hundreds of claims relating to vaccination-related injuries, which spiked in August when New Zealand’s Pfizer vaccine rollout was ramping up.
As of August 7, ACC had received 201 treatment injury claims related to the vaccine. Of those, 67 had been accepted, 39 declined and 95 were still being decided.
A month later (September 10), a further 181 claims had been received – a total of 382. Of these, 144 had been accepted, 73 declined and 163 were still being decided.
The majority of accepted claims were for allergic reactions.
Official documents that were meant to be kept secret have been released under the Freedom of Information Act, and they reveal that the forced euthanasia of the elderly and vulnerable in response to a pandemic had been years in the planning.
As soon as lockdown was declared in the United Kingdom on March 23rd 2020 deaths occurring in care homes in the weeks that followed skyrocketed compared to what had occurred in the previous five years. You were led to believe this was because of Covid-19, but the evidence shows otherwise.
4 British Airways Pilots Dead 5 Air India Pilots Dead 5 Jet Blue Pilots Dead 1 Canadian Cargo Pilot Dead
BREAKING NOW! Five Jet Blue Airlines pilots are confirmed dead, current Jet Blue pilot whistleblower confirms push for jab continues. Dr. Jane Ruby joins Stew Peters with details.
“Then God said, “I now give you every seed-bearing plant on the face of the entire earth and every tree that has fruit with seed in it. They will be yours for food.” – Genesis 1:29
Get Hydroxychloroquine (HCQ), Ivermectin, and other COVID-19 medications in the USA in almost every state within 24 hours —> https://deeprootsathome.com/an….alyze-risk-benefit-f Get COVID medication sent to your home —> CALL RAVKOO PHARMACY – Phone: 863-875-5700
Sometime after June 9, 2020 the WHO changed the definition of “herd immunity” from naturally acquried immunity or vaccinated immunity, to vaccinated ONLY immunity. I have “heard” immunity … I heard this is a scam-demic where the real purpose is to inject people with an Experimental Genetic Code so they can be culled and controlled! —> https://web.archive.org/web/20….201023093420/https:/
Health Freedom Advocacy Center – You can hold the government accountable to protect your ability to choose what’s best for your health and for the wellbeing of your children. —> https://standforhealthfreedom.com/
*LOTS OF LINKS* Medical Opposition to CoVid-19 LockDowns, Vaccine Dangers, Disturbing Global Agendas, 5G Radiation, Boost Immune System Naturally —> http://might-want-to-know.medianewsonline.com/
EWR Note: NZ (as with all other nations under the ‘spell’ of the globalists) is fully in step with the BBB scam. ‘Government remains focused on building back better’ (Hon Grant Robertson, Feb 2021). BBB even has a special NZ website here About Build Back Better: “While there has been some debate on the meaning and suitability of the phrase “Building Back Better”, we have embraced BBB as an important concept for pre- and post-disaster resilience building in-line with the United Nations, World Bank, and international researchers and authors including Clinton, Monday, Khasalamwa and Kennedy.”
“The coronavirus pandemic gives the world a chance to reset and ‘build back better'”, former Prime Minister Helen Clark says… (article & video at the link).
Dare I say it? Knowing what we do about man made disasters, this article from mercola.com rings very true. Remember the globalist ‘Lockstep’ plan? (Articles on that topic here).
Read the mercola article below:
Story at-a-glance
Top political figures and Big Tech leaders are using the common refrain that the COVID-19 pandemic has provided an opportunity to “reset” and “build back better”
Founder and executive chairman of the World Economic Forum (WEF) Klaus Schwab first started circulating the idea of The Great Reset, of which “build back better” is an integral part of
The COVID-19 pandemic is being used as a justification for the movement, but the agenda has nothing to do with health and everything to do with a long-term plan to monitor and control the world through technical surveillance
Citing pandemic-induced unemployment, record levels of global government debt and a shrinking world economy, Schwab warns that the COVID-19 crisis is going to exacerbate environmental issues and social crises, such as rising inequality
The reset solution is to “build entirely new foundations for our economic and social systems,” which everyone should adapt to since the pandemic has “shown how quickly we can make radical changes to our lifestyles”
“Building back better” envisions a world in which you’re tied to an electronic ID linked to your bank account and health records, have a “social credit” ID that can run every facet of your life and own no personal property
Top political figures and Big Tech leaders are using the common refrain that the COVID-19 pandemic has provided an opportunity to “reset” and “build back better.” But what does it really mean to “build back better”?
Founder and executive chairman of the World Economic Forum (WEF) Klaus Schwab first started circulating the idea of The Great Reset, of which “build back better” is an integral part.
“There is an urgent need for global stakeholders to cooperate in simultaneously managing the direct consequences of the COVID-19 crisis,” WEF states on their Great Reset website. So WEF started The Great Reset initiative as a method to “improve the state of the world.”1
It’s a lofty description but again one that actually tells you nothing. “Build back better” is a tagline of sorts for The Great Reset, and though this is being played off as a new initiative, it’s simply a rebranding of terms for technocracy and the old “New World Order.”
An elite oligarchy is behind this technocratic plan to govern society through technology, programmed by scientists and technicians and automated through the use of artificial intelligence, rather than through democratically elected politicians and government leaders.
COVID-19 Used to Justify the Need to ‘Build Back Better’
The current pandemic is being used as a justification for the movement, but the agenda has nothing to do with health and everything to do with a long-term plan to monitor and control the world through technical surveillance. As Schwab wrote, “There are many reasons to pursue a Great Reset, but the most urgent is COVID-19.”2
Citing pandemic-induced unemployment, record levels of global government debt and a shrinking world economy, Schwab warns that the COVID-19 crisis is going to exacerbate environmental issues and social crises, like rising inequality. The solution? “We must build entirely new foundations for our economic and social systems.”3 Fortunately, he writes, there is a silver lining to the pandemic and that is “it has shown how quickly we can make radical changes to our lifestyles.”4
This will be key to “building back better,” which envisions a world in which you’re tied to an electronic ID linked to your bank account and health records, and have a “social credit” ID that can run every facet of your life. Schwab detailed three main components of The Great Reset agenda:5
1. Steer the Market Toward “Fairer Outcomes” — “To this end, governments should improve coordination (for example, in tax, regulatory and fiscal policy), upgrade trade arrangements and create the conditions for a ‘stakeholder economy.’”
Also known as stakeholder capitalism, Forbes described stakeholder economy as “the notion that a firm focuses on meeting the needs of all its stakeholders: customers, employees, partners, the community and society as a whole.”6
The idea of stakeholder capitalism has been around since at least 1932, and was also endorsed by nearly 200 CEOs of large corporations in August 2019.7 However, it is now being accelerated as part of The Great Reset.
“At a time of diminishing tax bases and soaring public debt, governments have a powerful incentive to pursue such action,” Schwab wrote. “Moreover, governments should implement long-overdue reforms that promote more equitable outcomes. Depending on the country, these may include changes to wealth taxes, the withdrawal of fossil-fuel subsidies and new rules governing intellectual property, trade and competition.”8
Yet, as Forbes pointed out, forms of stakeholder capitalism have already been tried and failed, because balancing conflicting stakeholder claims was near-impossible and only led to mass confusion and poor returns. The failure of this strategy is what led big businesses to focus on maximizing shareholder value instead.
2. Ensure That Investments Advance Shared Goals — Shared goals, such as equality and sustainability, should be at the heart of government and private investments, and rather than funneling government recovery funds and economic-stimulus funding to “fill cracks in the old system,” these should be used to “create a new one that is more resilient, equitable and sustainable in the long run.”
Schwab added, “This means, for example, building ‘green’ urban infrastructure and creating incentives for industries to improve their track record on environmental, social, and governance (ESG) metrics.”9 It all sounds well and good, except, as Technocracy News reported in June 2020, “the promised Utopia comes with a price — it sets shackles on our personal freedom …”10
The required sacrifices do not apply to the technocrats running the system, so ultimately The Great Reset will result in two tiers or people: the technocratic elite, who have all the power and rule over all assets, and the rest of humanity, who have no power, no assets and no say-so in anything.
3. Harness the Innovations of the Fourth Industrial Revolution — The Fourth Industrial Revolution, which Schwab has been discussing since at least 2016,11 “is characterized by a fusion of technologies that is blurring the lines between the physical, digital and biological spheres.”
In terms of government, the Revolution will bring new technological powers that allow for increased population control via “pervasive surveillance systems and the ability to control digital infrastructure.”12 As for as its effects on people, Schwab writes:13
“The Fourth Industrial Revolution, finally, will change not only what we do but also who we are. It will affect our identity and all the issues associated with it: our sense of privacy, our notions of ownership, our consumption patterns, the time we devote to work and leisure, and how we develop our careers, cultivate our skills, meet people, and nurture relationships.
It is already changing our health and leading to a ‘quantified’ self, and sooner than we think it may lead to human augmentation. The list is endless because it is bound only by our imagination.”
Increased Surveillance Is Necessary for the Reset
The planned reform will affect everything from government, energy and finance to food, medicine, real estate, policing and even how we interact with our fellow human beings in general. Part of this involves increased surveillance, which is already being rolled out in the name of public health.
Vaccine passports are one example. Hastily ushered in as a byproduct of the COVID-19 pandemic, they’re expected to become “widely available” during the first half of 2021.14
If the initiative is successful, you’ll likely be required to pull up a vaccine certificate on your phone showing when and where you were vaccinated, along with which type of vaccine, in order to get on a plane or attend an indoor event, such as a concert, for starters.
WEF and the Commons Project created the Common Trust Network, which developed the CommonPass app that’s intended to act as a health passport in the near future. The app allows users to upload medical data such as a COVID-19 test result or proof of vaccination, which then generates a QR code that you will show to authorities as your health passport.15
The proposed common framework “for safe border reopening” around the world involves the following:16
Every nation must publish their health screening criteria for entry into the country using a standard format on a common framework
Each country must register trusted facilities that conduct COVID-19 lab testing for foreign travel and administer vaccines listed in the CommonPass registry
Each country will accept health screening status from foreign visitors through apps and services built on the CommonPass framework
Patient identification is to be collected at the time of sample collection and/or vaccination using an international standard
The CommonPass framework will be integrated into flight and hotel reservation check-in processes
Eventually, the CommonPass framework will be integrated with already existing personal health apps such as Apple Health and CommonHealth. If you want to travel, your personal health record will be evaluated and compared to a country’s entry requirements, and if you don’t meet them, you’ll be directed to an approved testing and vaccination location.
Privacy concerns are still being raised, however, which is why every effort is being made to get people to loosen their views on the right for privacy. In the U.S., there’s also the Constitution that stands in the way, which is why efforts to undermine, circumvent, ignore or nullify it are increasing.
Even Food Will Be Affected
For those who control resources like food, power is limitless, and control of the food supply is also part of “building back better.” WEF has partnered with the EAT Forum, which will set the political agenda for global food production. The EAT Forum was cofounded by the Wellcome Trust, which in turn was established with the financial help of GlaxoSmithKline.
EAT collaborates with nearly 40 city governments across Africa, Europe, Asia, North and South America and Australia, and maintains close relationships with imitation meat companies such as Impossible Foods, which was co-funded by Google, Jeff Bezos and Bill Gates.17
Bill Gates, by the way, owns more farmland in the U.S. than any other private farmer, having purchased a total of 242,000 acres — much of it considered some of the richest soil in the country — in the past few years.18 Gates is also a supporter of The Great Reset,19 which is curious since his massive accumulation of wealth and land is the opposite of what the Great Reset promotes.
In truth, wealthy technocrats will not redistribute their own wealth during the reset, but will only continue to grow their financial empires as the rest of the world consents to giving up their privacy and ownership of all property.20
EAT developed a “Planetary Health Diet” that is designed to be applied to the global population and entails cutting meat and dairy intake by up to 90%, replacing it largely with foods made in laboratories, along with cereals and oil.21
They Don’t Want to Return to Normal
Many people around the world are counting down the days until the COVID-19 pandemic is over and life can return to normal. But the very purpose of “building back better” is to do away with what was once “normal” and replace it with something different. According to WEF, this entails “reinventing capitalism”:22
“A true recovery from COVID-19 will not be about putting things back together the way they were: we need to ‘build back better’, to ‘reset’, if we are to address the deep systemic vulnerabilities the pandemic has exposed.
… If we don’t seize this opportunity to build back better – to reset and reinvent rather than ‘return to normal’ – systemic risks and vulnerabilities will continue to accumulate, making future shocks both more likely and more dangerous.
Despite the tragedy, we must leverage the COVID-19 pandemic, and make sure that it becomes the catalyst for a profoundly positive transformation of the global economy, taking us closer to a world in which everyone can live well, within planetary boundaries.”
The warning signs are all around, for those willing to see them for what they actually are — an unprecedented effort to monitor, modify and control human behavior disguised as pandemic relief.
Greece has become the latest European country to be hit with mass protests after the government announced the unvaccinated would be banned from visiting bars, restaurants, cinemas and other public places.
Thousands of demonstrators descended on Athens and Thessaloniki, with crowds chanting “Hands off our kids!” and holding signs that said “We say no to vaccine poison.”
All nursing home staff and hospital workers will be mandated to get the vaccine from August 16, while hospital workers also face losing their jobs unless they get the compulsory jab from September.
And, from this, Israel’s “health” authorities conclude that the solution (final?) is more “vaccination.”
“Our free press” continues to (a) black out the fact that most of those who have fallen ill, allegedly with COVID-19, were “vaccinated,” while (b) spreading the Big Lie, enabled by the CDC’s cooked numbers, that the opposite is true.
That’s not just propaganda, but propaganda at its most poisonous, as it’s laying the psychic groundwork for what’s coming next (if They should have Their way): scapegoating of the “unvaccinated,” followed by their forcible injection and/or mass arrest.
In light of what’s at stake, we need strong and unrelenting protest, not of any state or federal “health” agencies, but of the media outlets blacking out the truth with that Big Lie. Their offices and networks should be hit with (peaceful) protests that they can’t ignore.
From David Diamond:
A vaccinated kid infects 83 mostly vaccinated kids at a party. The virus is traced to his vaccinated uncle and then to another vaccinated carrier.
If this is 95% efficacy, I hate to see what would happen if the vax didn’t work.
By the way, the conclusion of the Israeli health authorities was more vaccination.
An interview from James Delingpole. An inside commentary on life in the medical practice in which the interviewee works. The phenomenal numbers of adverse reactions you aren’t hearing about from mainstream. The deaths. The injured patients who show up for post-cv-vx help & are persuaded by their Doctor it ‘is not the vx’. MDs he has lost all respect for. A must hear… listen at the link:
UK Dr, Samuel White has resigned, sick of the lies & cover up. The cures suppressed, the unnecessary deaths. The real risks of the jab and what it really is. A short 7 min or less watch. Vital, crucial info for you. This is a medical doctor who like many others now is taking his pledge of ‘do no harm’ with great seriousness. Please listen. There are three links. The Instagram is the longest, fb and twitter are condensed. Links below:
As a result of the government’s post VX Challenge so called emergency “technical” law change, any VX or other medicine can now be approved at the Minister’s discretion for everyone in NZ, based on an application that ONLY considers (a) to (h) below.
The Minister need NOT consider (i) to (p) which assess SAFETY, integrity and EFFICACY.
How can the govt adverts properly claim provisional consent from Medsafe means this novel jab is “safe and effective”. It’s now a “Clayton’s” Medicines Act that depending on the Minister’s whim protects nobody from anything…..
Comments by Brian Shilhavy Editor, Health Impact News
The Standard, Hong Kong’s biggest circulation English daily newspaper, is reporting that 12 people have died, and 4 women have had miscarriages following COVID-19 shots just in the past week.
For the past week between May 24 and 30, 12 more people died at public hospitals after receiving the Covid vaccines, along with four women who suffered from miscarriages, according to the Hospital Authority.
The Hospital Authority said six of the 12 cases were hospitalized patients while the rest passed away in the emergency department.
With the additional miscarriage cases, Hong Kong has now seen 23 miscarriage cases after vaccination.
From February 26, when the city’s vaccination campaign started, until last Sunday, the city recorded 80 deaths following vaccinations.
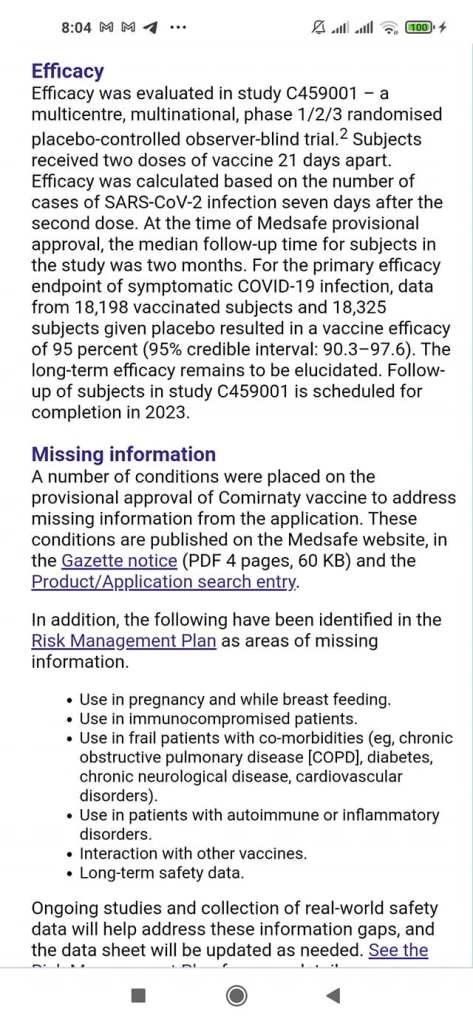
On 3 June Medsafe belatedly published a summary of some of the outstanding safety and efficacy Information about the Pfizer jab. This important information should be included in ALL informed consent conversations and ALL employer/ employee health and safety discussions https://www.medsafe.govt.nz/…/Spotlight-on-Comirnaty…NB what they still don’t say is that the benefit/risk assessment required for s23(1) considers mainly administrative type Information and does NOT include assessment of product safety, integrity or efficacy (that is why this process was only available for the restricted treatment of a limited number of patients until the govt passed an emergency law on 19 May 2021 to retrospectively validate this and a few other novel medicines which had incomplete safety testing).
EWR Note: for the FDA’s list of more than thirty possible side effects also not included in information supplied in NZ go to this link, at page 17.
Summarised below:
KNOWN POSSIBLE SIDE EFFECTS FROM THE COVID-19 EXPERIMENTAL mRNA INJECTION This is a draft list compiled by the FDA – the Food and Drug Administration in the US:
Authorities in Denmark have shut down much of the country’s access to video platform Bitchute in the name of preventing the spread of “dangerous information” about COVID.
Denmark’s National Police Cyber Crime Center (NC3) petitioned for a court order to block the site and ISPs followed suit by blocking access to users.
“The National Police Cyber Crime Center (NC3) has blocked the homepage that your browser has tried to access contact as there is reason to assume that from the website commits a violation of criminal law, which has a background in or connection with the covid-19 epidemic in Denmark,” states a message users see when trying to access Bitchute.
It then advises the owner of the website that they will have to contact the authorities in order to try to get the website back online.
“The block appears to be site-wide meaning that Danish citizens aren’t just being prevented from viewing alleged COVID-19 misinformation on BitChute – they’re being blocked from viewing any BitChute videos, regardless of the topic,” writes Tom Parker.
Comments by Brian Shilhavy Editor, Health Impact News
Last month we published an interview with Dr. Charles Hoffe, a medical doctor for 28 years in the small, rural town of Lytton in British Columbia, Canada.
He tried to sound the alarm over the troubling side effects he was seeing in his community from the COVID-19 shots, which included one death.
The results of his trying to warn the medical system about what he was seeing are that he was issued a gag order and basically told to shut up.
He didn’t. He did an interview explaining what was happening after the COVID-19 shots, and the damage they were causing, putting his own career on the line. See:
LifeSite News is now reporting that Dr. Hoffe was relieved of his emergency room duties, which has resulted in him losing half of his income, because he dared to tell the truth.
Canadian doctor removed from hospital duty after speaking out about COVID vaccine side effects
A Canadian family doctor says he has been punished by his local health authority because he raised concerns about side effects he observed in some of those who had received the Moderna COVID-19 jab within his community.
“I am no longer allowed to work in the ER,” British Columbia Dr. Charles Hoffe said, according to a True North News report.
Hoffe added that his suspension from the ER came at the end of April, after his local health authority “suspended” his clinical privileges “for the crime of causing ‘vaccine hesitancy,’ for speaking out about my vaccine injured patients.”
In an April 5 letter, Hoffe had written to British Columbia Provincial Health Officer Bonnie Henry that he was “quite alarmed at the high rate of serious side effects from this novel treatment,” in reference to Moderna COVID-19 injections given to 900 mostly Indigenous people in Lytton, British Columbia.
Hoffe said he had observed one patient death, “numerous” allergic reactions, along with three individuals who had “disabling” neurological deficits completed with chronic pain, which persisted “for more than 10 weeks after their first vaccine.”
“So in short, in our small community of Lytton, BC, we have one person dead, and three people who look as though they will be permanently disabled, following their first dose of the Moderna vaccine. The age of those affected ranges from 38 to 82 years of age,” wrote Hoffe.
Following his letter, Hoffe said, he is no longer allowed to work in the ER department of St. Bartholomew’s Health Centre due to his views on the COVID injection. He still can work in his private practice.
“I am still permitted to see patients in my private practice, which is not under the jurisdiction of the Interior Health authority,” Hoffe said.
Losing the ability to work in the ER has resulted in his income being slashed by half, which he explained is “the price of advocating for the safety of my patients.”
Dear Prime Minister, Attorney-General, Minister of Health, Minister of Covid, Minister or Seniors, Director General of Health and Chris Hipkins. I attach below some new and very important research which I must assume your advisors have not yet provided to you, or the experimental Pfizer injection rollout would surely already have been suspended. It is now clearly established that the SProtein is a toxin that causes the harmful symptoms known as “Covid”.
I surely don’t need to explain the legal, ethical and human rights consequences of a government knowingly promoting a program which intentionally injects a life threatening toxin into healthy people. I also attach a report indicating that injected nanoparticles (and the SProtein) do not remain in the arm muscle but instead circulate throughout the whole body. The combined effect is that the Pfizer jab injects mRNA to take over cells to manufacture the deadly SProtein toxin and this spread throughout much of the body, manufacturing the SProtein toxin for days and in some cases many weeks. This explains why even the limited available research from the two months of study as summarised in the Comirnaty Data Sheet identifies possible harm to many different parts of the body including the heart, blood, brain, musculoskeletal system, nervous system, fainting and dizziness etc. This is no longer just a shocking experiment. Everyone involved is now on notice of this “injection roulette” which may result in death or serious injury to previously healthy people. The health and safety implications for employers and those who push this jab, are significant. No post injection death can legitimately be ruled out as being caused or contributed by the injection, at least not without a full coroner’s report. Certainly any post vax stroke, heart attack, other blood disorder, nervous system disorder or even suicide or car accident (known overseas as “vaccidents”) must prima facie be assumed to be caused or contributed to by the jab, at least until a full coroners report is undertaken. Similarly it is not good enough to claim that our seniors who die post jab were frail and likely to die. Surely if they were that frail they should have been spared from the jab. Anyway, surely “deaths post Jab” should be treated consistently with “deaths post Covid”. Despite the secretive, flawed and very passive official post jab injury reporting process ( CARM), and as a result of the more active community led follow up, you are already on notice of a number of deaths and life threatening and life changing harm from this injection. The deaths and harm will inevitably continue if there are any further injections. Perhaps initially you had an excuse that you thought the SProtein was “safe”. However now you are on notice that it is not “safe” by any definition. Further, although you in privileged position are on notice, many members of the public who you were elected to represent remain deceived by misleading claims in crown propaganda that the jab is “safe and effective”. In these circumstances there can be no “Informed consent”., Each jab without Informed consent is in breach of the Health and Disability Code and is an assault. In these circumstances, the ongoing program is surely criminal, and indeed may result in Homicide as defined by the Crimes Act: 158Homicide defined Homicide is the killing of a human being by another, directly or indirectly, by any means whatsoever. Compare: 1908 No 32 s 173 Anyone who aids, abets or otherwise incites homicide is a party to that homicide. I note that the Director-General of Health has shared his view in sworn evidence that Covid is the most serious health issue for New Zealand in 100 years. I invite you all to consider that claim very carefully and critically. Please put Covid in perspective against the many other challenges which we face, including for example heart attacks, strokes, cancer, suicide accidents and diabetes and the nitrate and other contamination of much of our water. Surely you must agree that the harm is not from “Covid” but from the “Response to Covid”. The best expert evidence is that the risk from Covid is similar to the risk from influenza. Many experts are now saying that Covid is simply a rebranding of influenza and colds, supported by PCR testing that was never intended as a diagnostic tool. The WHO says that PCR testing should not be used beyond 20-25 cycles. OIA responses indicate that in NZ PCR tests use up to 45 cycles, which simply multiplies any contamination. Our government is about to enter dangerous new phase if it proceeds to inject more healthy New Zealanders with an injection that experts have established is toxic. Apart from the direct harm to those who choose, or are bullied to accept this injection, there is considerable peripheral harm. This includes the contamination of our Blood Bank with SProtein. We can only speculate on the risks for vulnerable people who receive blood contaminated with this toxin. Please stop and reflect. Please listen to international experts who are independent from Big Pharma and who are not invested in the Covid paradigm. Please listen to the New Zealand scientific and medical experts who have put their careers and reputations on the line out of extreme concern. Please correct the misinformation that this injection is “safe and effective” and “approved by Medsafe” when in fact it did not meet the statutory criteria that “benefit exceeds risk”. There is no imminent health risk from suspending the program. Dr Bloomfield’s sworn evidence was that the risks were mainly financial and reputational. Please find the courage to challenge whoever is driving this, and any who act on dogma rather than evidence, reason or ethics. The future of New Zealand depends on your courage to step up and make this critical call for our people. I urge you to listen, engage and act in the public interest. Please put aside your pride and the dogma, and suspend this program. I am happy to assist however I can.
Sue Grey LLB (Hons), BSc (Biochemistry and Microbiology), RSHDipPHI Co-leader NZ Outdoors Party suegreylawyer@gmail.com sue.grey@outdoorsparty.co.nz
We wish to notify you of our grave concerns regarding all proposals to administer COVID-19 vaccines to children. Recently leaked Government documents suggested that a COVID-19 vaccine rollout in children over 12 years old is already planned for September 2021, and the possibility of children as young as 5 years old being vaccinated in the summer in a worst-case scenario.1
We have been deeply disturbed to hear several Government and SAGE representatives calling in the media for the COVID-19 vaccine rollout to be “turning to children as fast as we can”.2 Teaching materials circulated to London schools contain emotionally loaded questions and inaccuracies3. In addition, there has been disturbing language used by teaching union leaders, implying that coercion of children to accept the COVID-19 vaccines through peer pressure in schools was to be encouraged, despite the fact that coercion to accept a medical treatment is against UK and International Laws and Declarations.4 Rhetoric such as this is irresponsible and unethical, and encourages the public to demand the vaccination of minors with a product still at the research stage and about which no medium- or long-term effects are known, against a disease which presents no material risk to them. A summary of our reasons is given below and a more detailed fully referenced explanation is available.5
Risks and benefits in medical treatments Vaccines, like any other medical treatment, come with varied risks and benefits. Therefore, we must consider each product, individually, on its merits, and specifically for which patients or sections of the population is the risk/benefit ratio acceptable. For COVID-19 vaccines, the potential benefits are clear for the elderly and vulnerable, however, for children, the balance of benefit and risk would be quite different. We are raising these concerns as part of an informed debate, which is a vital part of the proper, scientific process. We must ensure that there is no repeat of any past tragedies which have occurred especially when vaccines are rushed to market. For example, the swine flu vaccine, Pandemrix, rolled out following the pandemic of 2010, resulted in over one thousand cases of narcolepsy, a devastating brain injury, in children and teenagers, before being withdrawn.6 Dengvaxia, a new vaccine against Dengue, was also rolled out to children ahead of the full trial outcomes, and 19 children died of possible antibody dependent enhancement (ADE) before the vaccine was withdrawn.7 We must not risk a repeat of this with the COVID-19 vaccines, which would not only impact on the children and families affected, but would also have a hugely damaging effect on vaccination uptake in general.
No medical intervention should be introduced on a ‘one size fits all’ basis, but instead should be fully assessed for suitability according to the characteristics of the age cohort and of the individuals concerned, weighing up the risk versus benefit profile for each cohort and the individuals within a group. This approach was outlined last October, by the head of the Government Vaccine Task Force, Kate Bingham, who said “We just need to vaccinate everyone at risk. There’s going to be no vaccination of people under 18. It’s an adult-only vaccine, for people over 50, focusing on health workers and care home workers and the vulnerable.”8
Children do not need vaccination for their own protection Healthy children are at almost no risk from COVID-19, with risk of death as low as 1 in 2.5 million9. No previously healthy child under the age of 15 died during the pandemic in the UK and admissions to hospital or intensive care are exceedingly rare10 with most children having no or very mild symptoms. Although Long-Covid has been cited as a reason for vaccinating children, there is little hard data. It appears less common and much shorter-lived than in adults and none of the vaccine trials have studied this outcome11 12. The inflammatory condition, PIMS, was listed as a potential adverse effect in the Oxford AstraZeneca children’s trial13. Naturally acquired immunity will give broader and better lasting immunity than vaccination14. Indeed, many children will already be immune15. Individual children at very high risk can already receive vaccination on compassionate grounds16.
Children do not need vaccination to support herd immunity Already, two thirds of the adult population have received at least one dose of a COVID-19 vaccine17. Models that assume vaccination of children is required to reach herd immunity have failed to account for the proportion who had immunity prior to March 2020 and those who have acquired it naturally18. Recent modelling suggested that the UK had achieved the required herd immunity threshold on 12 April 2021.19
Children do not transmit SARS-CoV-2 as readily as adults, moreover adults living or working with young children are at lower risk of severe COVID-1920. Schools have not been shown to be the focus on spread to the community, teachers have a lower risk of COVID-19 than other working age adults21.
Short-term safety concerns As of 13th May, the MHRA22 has received a total of 224,544 adverse events, including 1,145 deaths in association with SARS-CoV-2 vaccines. Reports of strokes due to cerebral venous thromboses were initially in low numbers but as awareness increased, many more reports led to the conclusion that AstraZeneca vaccine should not be used for adults under 40 years of age and this unpredicted finding has also led to the suspension of the Oxford AstraZeneca children’s trial.
Similar events have been noted with Pfizer & Moderna vaccines on the US adverse reporting system (VAERS)23 and it is likely that this is a class effect related to production of spike protein. New UK guidelines on managing Vaccine-Induced Thrombotic Thrombocytopenia (VITT)24 include all COVID-19 vaccines in their advice. The possibility of further unexpected safety issues cannot be ruled out. In Israel, where the vaccines have been widely rolled out to young people and teenagers, the Pfizer vaccine has been linked to several cases of myocarditis in young men25 and concerns have been raised about reports of altered menstrual cycles and abnormal bleeding in young women following the vaccine.26
Most concerning with regard to possible vaccination of children, is that there have now been a number of deaths associated with vaccination reported to VAERS in the US, despite the vaccines only being given to children within trials and a very recent rollout to 16-17 year olds27.
Long-term safety concerns All Phase 3 COVID-19 vaccine trials are ongoing and not due to conclude until late 2022/early 2023. The vaccines are, therefore, currently experimental with only limited short-term and no long-term adult safety data available. In addition, many are using a completely new mRNA vaccine technology, which has never previously been approved for use in humans28. The mRNA is effectively a pro-drug and it is not known how much spike protein any individual will produce. Potential late-onset effects can take months or years to become apparent. The limited children’s trials undertaken to date are totally underpowered to rule out uncommon but severe side effects.
Children have a lifetime ahead of them, and their immunological and neurological systems are still in development, making them potentially more vulnerable to adverse effects than adults. A number of specific concerns have been raised already, including autoimmune disease and possible effects on placentation and fertility.29 A recently published paper raised the possibility that mRNA COVID-19 vaccines could trigger prion-based, neurodegenerative disease30. All potential risks, known and unknown, must be balanced against risks of COVID-19 itself, so a very different benefit/risk balance will apply to children than to adults.
Conclusion There is important wisdom in the Hippocratic Oath which states, “First do no harm”. All medical interventions carry a risk of harm, so we have a duty to act with caution and proportionality. This is particularly the case when considering mass intervention in a healthy population, in which situation there must be firm evidence of benefits far greater than harms. The current, available evidence clearly shows that the risk versus benefit calculation does NOT support administering rushed and experimental COVID-19 vaccines to children, who have virtually no risk from COVID-19, yet face known and unknown risks from the vaccines. The Declaration of the Rights of the Child states that, “the child, by reason of his physical and mental immaturity, needs special safeguards and care, including appropriate legal protection”.31 As adults we have a duty of care to protect children from unnecessary and foreseeable harm.
We conclude that it is irresponsible, unethical and indeed, unnecessary, to include children under 18 years in the national COVID-19 vaccine rollout. Clinical trials in children also pose huge ethical dilemmas, in light of the lack of potential benefit to trial participants and the unknown risks. The end of the current Phase 3 trials should be awaited as well as several years of safety data in adults, to rule out, or quantify, all potential adverse effects.
We call upon our governments and the regulators not to repeat mistakes from history, and to reject the calls to vaccinate children against COVID-19. Extreme caution has been exercised over many aspects of the pandemic, but surely now is the most important time to exercise true caution – we must not be the generation of adults that, through unnecessary haste and fear, risks the health of children.
Signatories
Dr Rosamond Jones, MD, FRCPCH, retired consultant paediatrician Lord Moonie, MBChB, MRCPsych, MFCM, MSc, House of Lords, former parliamentary undersecretary of state 2001-2003, former consultant in Public Health Medicine Prof Anthony Fryer, PhD, FRCPath, Professor of Clinical Biochemistry, Keele University Professor Karol Sikora, MA, MBBChir, PhD, FRCR, FRCP, FFPM, Dean of Medicine, Buckingham University, Professor of Oncology Professor Angus Dalgleish, MD, FRCP, FRACP, FRCPath, FMed Sci, Professor of Oncology, St Georges Hospital London Professor Richard Ennos, MA, PhD. Honorary Professorial Fellow, University of Edinburgh Professor Anthony J Brookes, Department of Genetics & Genome Biology, University of Leicester Professor Keith Willison, PhD, Professor of Chemical Biology, Imperial, London Dr John A Lee, MBBS, PhD, FRCPath, retired Consultant Histopathologist, former Clinical Professor of Pathology at Hull York Medical School Dr Alan Mordue, MBChB, FFPH (ret). Retired Consultant in Public Health Medicine & Epidemiology Dr Elizabeth Evans, MA, MBBS, DRCOG, retired doctor Mr Malcolm Loudon, MB ChB, MD, FRCSEd, FRCS (Gen Surg). MIHM, VR. Consultant Surgeon Dr Gerry Quinn, PhD, Microbiologist Dr C Geoffrey Maidment, MD, FRCP, retired consultant physician Dr K Singh, MBChB, MRCGP, general practitioner Dr Pauline Jones MB BS retired general practitioner Dr Holly Young, BSc, MBChB, MRCP, Consultant physician, Croydon University Hospital Dr David Critchley, BSc, PhD, 32 years in pharmaceutical R&D as a clinical research scientist. Dr Padma Kanthan, MBBS, General practitioner Dr Thomas Carnwath, MBBCh,MA, FRCPsych, FRCGP, consultant psychiatrist Dr Sam McBride BSc(Hons) Medical Microbiology & Immunobiology, MBBCh BAO, MSc in Clinical Gerontology, MRCP(UK), FRCEM, FRCP(Edinburgh). NHS Emergency Medicine & geriatrics Dr Helen Westwood MBChB MRCGP DCH DRCOG, general practitioner Dr M A Bell, MBChB, MRCP(UK), FRCEM, Consultant in Emergency Medicine, UK Mr Ian F Comaish, MA, BM BCh, FRCOphth, FRANZCO, Consultant ophthalmologist Dr Jayne LM Donegan MBBS, DRCOG, DCH, DFFP, MRCGP, general practitioner Dr Dayal Mukherjee, MBBS MSc Dr Clare Craig, BM,BCh, FRCPath, Pathologist Mr C P Chilton, MBBS, FRCS, Consultant urologist emeritus Dr Theresa Lawrie, MBBCh, PhD, Director, Evidence-Based Medicine Consultancy Ltd, Bath Dr Jason Lester, MRCP, FRCR, Consultant Clinical Oncologist, Rutherford Cancer Centre, Newport Dr Scott McLachan, FAIDH, MCSE, MCT, DSysEng, LLM, MPhil., Postdoctoral researcher, Risk & Information management Group Michael Cockayne, MSc, PGDip, SCPHNOH, BA, RN, Occupational health practitioner Dr John Flack, BPharm, PhD. Retired Director of Safety Evaluation at Beecham Pharmaceuticals 1980-1989 and Senior Vice-president for Drug Discovery 1990-92 SmithKline Beecham Dr Stephanie Williams, Dermatologist Dr Greta Mushet, retired Consultant Psychiatrist in Psychotherapy. MBChB, MRCPsych Dr JE, MBChB, BSc, NHS hospital junior doctor Mr Anthony Hinton, MBChB, FRCS, Consultant ENT surgeon, London Dr Elizabeth Corcoran,MBBS,MRCPsych,Psychiatrist,Chair Down’s Syndrome Research Foundation UK Dr Alan Black, MB BS MSc DipPharmMed, retired pharmaceutical physician Dr Christina Peers, MBBS,DRCOG,DFSRH,FFSRH, Consultant in Contraception & Reproductive Health Dr Marco Chiesa, MD, FRCPsych, Consultant Psychiatrist & Visiting Professor, UCL Elizabeth Burton, MB ChB, retired general practitioner Noel Thomas, MA, MB ChB, DCH, DObsRCOG, DTM&H, MFHom, retired doctor Malcolm Sadler, MBBS, FRCGP, retired general practitioner with 37 years in Medical Practice Dr Ian Bridges, MBBS, Retired general practitioner Mr T James Royle MBChB, FRCS(Ed), MMedEd, Consultant colorectal surgeon Dr Fiona Martindale, MbChB, MRCGP, GP in out of hours









































You must be logged in to post a comment.