It is tempting to think of evil in apocalyptic imagery: vast and sudden demolition, a searing propulsive darkness or a blinding conflagration, the work of engineered catastrophic mayhem, in whose wake is utter smouldering demise. Yet the work of evil is often piecemeal, steady, methodical, and the accomplishment of a great wrong may well be the result of the gradual accumulative weight of small decisions, whose progress is all the surer for its studied implacability. I think of a large battalion of infantry moving painstakingly across a terrain and claiming it inch by inch until they have vanquished all. Yet, in truth, evil is varied, its manifestations as many as there are living human entities who, faced with seemingly slight or casual choices, often land on the side of self-interest, self-aggrandizement and deception. And evil, however disguised, appears in language.
NewZealandDoc’s Newsletter is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
You will forgive me this preface as I alight on a matter that demonstrates with simple clarity a facet of the evil that has been visited upon us during the Corona War by an institution purporting to have as its charge the protection of the public weal in its regulation of medical practitioners: the infamous Medical Council of New Zealand.
On 5 December 2019, while in the employ as a psychiatrist of one of New Zealand’s District Health Boards (since amalgamated into an overarching bureaucratic entity now known as Te Whatu Ora), I received an email communication about informed consent. The document can be perused in its entirety here:
The “Updated statement on informed consent,” signed by Chief Executive Officer Joan Simeon –now, coincidentally enough, the Chair of the Federation of State Medical Board’s international arm, the International Association of Medical Regulatory Agencies – states the following:
“The key points about informed consent are:
•Every time treatment is provided, a doctor must have permission to provide that treatment. The process of obtaining that permission is called ‘informed consent’. Without informed consent, the treatment may be unlawful. To help the patient decide whether they want a treatment, they first need to be given information, such as the risks and benefits of their treatment options.
•Obtaining consent is a process of shared decision-making where a doctor helps the patient understand their medical condition and the options for treating (or not treating) that condition. It is more than signing forms and completing paperwork. As a doctor, you need to take the time to ask questions so that you understand what matters to your patient, and what their concerns, wishes, goals and values are.”
Bear in mind that this statement, meant to be a standard of good medical practice and to be used as a measure of professional conduct, appeared just as covid had been unleashed upon the world.
Then, on 28 April 2021, this very same Medical Council, in conjunction with the Dental Council, issued a guidance statement on professional responsibility and the Covid-19 vaccine (so-called), which can be found here. It was withdrawn without fanfare on 13 September 2023. It is a masterpiece of obfuscation and an inversion of true informed consent. As such, it represents one of those unheralded but highly effective acts of evil.
Guidance Statement Covid 19 Vaccine And Your Professional Responsibility
Not only are health practitioners themselves expected to get the jab, but the regulators write that “it is our view that there is no place for anti-vaccination messages in professional health practice, nor any promotion of antivaccination claims including on social media and advertising by health practitioners,” while simultaneously advising that “As a health practitioner, you have a role in providing evidence-based advice and information about the COVID-19 vaccination to others. You should be prepared to discuss evidence-based information about vaccination and its benefits to assist informed decision making.”
Yet when one of my colleagues undertook to provide advice to a pregnant woman about medical issues connected with the use of the Pfizer inoculation, his licence was suspended. Furthermore, given the provisional approval of the inoculation at the time and the absence of long-term safety data, the much-vaunted informed consent process and the collaborative partnership with patients implied necessitated a frank discussion of serious risk – risk that has, sadly enough, been borne out not only in New Zealand but world-wide, with an extraordinary panoply of adverse events, including death, amounting to a genocide.
With every day each of us is confronted by choice, on matters small or large. However mauled we may or may not be by spike proteins, jabs, hippocampal lesions, or the weight of the massive psychological operation played against us with covid, we retain the freedom to choose. During the Holocaust perpetrated by Nazi Germany – in an era far before viral or vaccine-mediated bioweapons were in play – ordinary people made choices, bureaucrats made choices, neighbors made choices, and a tremendous evil was allowed to grow to a horrific immensity.
Undermining a real, a true, a genuine foundational principle of Medicine – informed consent – in the service of … of following an agenda that has oppressed and is still oppressing us and destroying viable and decent Medicine in the process, is but another one of those examples of how evil wins its way in our world. The Medical Council of New Zealand, ostensible protector of public health, has in its serpentine and devious manner, shown us that it is as destructive as it is hypocritical, and as corrupt as it is authoritarian.
And those many doctors out there who knew then and now know even better about their profession need to come out of hiding, no matter how uneasy or fearful of the “authorities” they may feel.
Unless they do so a medical profession worth keeping won’t be left.
I found it. A single question: “If the COVID vaccine is safe, can you explain this to me?” What happens is they respond with ad hominem attacks. They cannot answer this question. Ever.
Executive summary
The one question they can’t answer has been found.
They will either change the topic or start telling you how stupid you are.
The question: “If the COVID vaccine is so safe, how do you explain Fig 1 in this article?”
Background
I want to thank Dr. Graham Bottley for inspiring this. I finally have a single simple question that every mainstream doctor will run from.
Bottley is a “scientist” whose credentials are so formidable (in his own view), that he does not have to answer any questions. I asked him two softball questions and he avoided answering them and instead requested that I answer HIS question. I said “happy to, right after you answer my question.”
NOTE: Due to censorship Dr Mercola’s articles are archived to paid sub soon after publication, in which case the source link may no longer work. The article however is republished here in its entirety. EWR
Story at-a-glance
The 2023 omnibus appropriations bill includes 19 lines that could give the U.S. Food and Drug Administration the power to ban off-label use of approved medications
If the little-noticed provision is passed, doctors’ ability to freely treat patients, and patients’ ability to use all available treatments after making an informed decision, will be lost
The amendment puts the FDA, and by proxy Big Pharma, at the helm of powerful health care decisions that should be made on an individual, personalized level between a patient and their health care provider
In California, law AB 2098, which went into effect January 1, 2023, gives the state power to take away doctors’ medical licenses if they spread “misinformation” that goes against the standard COVID-19 rhetoric
The trend to allow a Pharma-controlled government to silence your doctor and dictate basic components of your medical care is not confined to the U.S. — it’s happening globally
In the U.S., 1 in 5 prescriptions is written for an off-label use.1 While sometimes this allows medications to be overused or misused, it also protects doctors’ ability to freely treat patients, and patients’ ability to use all available treatments after making an informed decision.
That 20% of medications are used off-label also indicates “a degree of freedom physicians currently have that will be foreclosed,” notes English comedian and actor Russell Brand,2 if a little-noticed provision in the omnibus spending bill is passed. “Literally, this will mean that your doctor will not be able to do what’s best for you because they’ll work for Big Pharma now,” Brand says.3
19 Lines in 4,155-Page Bill Could Change Practice of Medicine
The 2023 omnibus appropriations bill — a 4,155-page tome involving $1.7 trillion in spending — includes 19 lines that could give the U.S. Food and Drug Administration the power to ban off-label use of approved medications. In a commentary for The Wall Street Journal, Dr. Joel Zinberg wrote:4
“Physicians routinely prescribe drugs and employ medical devices that are approved and labeled by the Food and Drug Administration for a particular use. Yet sometimes physicians discern other beneficial uses for these technologies, which they prescribe for their patients without specific official sanction.
The new legislation amends the Food, Drug and Cosmetic Act, or FDCA, to give the FDA the authority to ban some of these off-label uses of otherwise approved products. This unwarranted intrusion into the physician-patient relationship threatens to undermine medical innovation and patient care.”
FDA Wants Power to Regulate Practice of Medicine
“The new provision was enacted at the FDA’s urging,” Zinberg says,5 in response to a 2021 legal ruling that limited the FDA’s power to meddle with the practice of medicine. In March 2020, the FDA banned the use of electric shock devices for particular uses, namely to treat patients engaging in self-harm or aggressive behaviors that could harm others.
The devices are FDA approved, and while the FDA banned their use for certain contexts, it still allowed them to be used for smoking addiction and other purposes.6 This led to a lawsuit — Judge Rotenberg Education Center v. FDA — in which the Judge Rotenberg Education Center, a school for people with severe behavioral and intellectual conditions, sued the FDA over the ban.
The court ruled in the school’s favor, stating that the FDA’s ban violated federal law because it interfered with health care practitioners’ authority to practice medicine. As it stands, the FDA does not have the power to ban medical devices for a particular use.
The school’s attorney, Mike Flammia, who also represented students’ parents in favor of the device’s use, told CNN the decision “protects what all of us cherish, and that is the ability to go to our doctor and have our doctor decide what is the best treatment.”7
As it stands, Section 360f of the FDCA8 only gives the FDA authority to ban a medical device if it poses “an unreasonable and substantial risk of illness or injury.” It can ban the device outright, but it can’t pick and choose when it can and can’t be used.
“Barring a practitioner from prescribing or using an otherwise approved device for a specific off-label indication would violate another FDCA section, which bars the FDA from regulating the ‘practice of medicine,'” Zinberg says.9 The FDA is trying to change that.
Pharma — Not Your Doctor — Would Dictate Medical Decisions
The omnibus amendment would change Section 360f so that the FDA could ban a medical device if it poses an unreasonable risk for “one or more intended uses” while leaving it approved for others. “Since the new provision lets the FDA skirt the ban on interfering with the practice of medicine by banning devices for particular uses, the agency will likely claim this as a precedent allowing it to ban off-label uses of drugs as well,” according to Zinberg.10
This puts the FDA, and by proxy Big Pharma, at the helm of powerful health care decisions that should be made on an individual, personalized level between a patient and their health care provider.
Remember that in 1992, the Prescription Drug User Fee Act (PDUFA) was created, which allows the FDA to collect fees from the drug industry. “With the act, the FDA moved from a fully taxpayer funded entity to one supplemented by industry money,” a BMJ article written by investigative journalist Maryanne Demasi explains.11
Now, significant portions of regulatory agencies’ budgets come from the pharmaceutical industry that these agencies are supposed to regulate. In 1993, after PDUFA was passed, the FDA collected about $29 million in net PDUFA fees. This increased 30-fold — to $884 million — by 2016.12
It’s also revealing that at the FDA, 9 out of 10 of its former commissioners between 2006 and 2019 went on to work for pharmaceutical companies.13 As Brand noted:14
“What they’re looking for is a crafty, sly, insidious way to be able to intercede in your relationship with your physician. And as usual, it’s for your ‘safety’ and for your ‘benefit’ … Why would you want Big Pharma and a regulatory body that they fund interfering in your relationship with your doctor about your health?
Have they not found enough ways to extract revenue from you, to put your health second, to put your well-being way, way behind their profits and their list of priorities? Why is the bias moving even further in that direction? … This is not about medicine. This is about licensing. This is about profits, patents, the ability to extract revenue.”
Patients Suffer When Pharma’s in Control
During the pandemic, it became clear how patients suffer when health agencies are allowed to dictate what medications doctors are allowed to prescribe to their patients. Ivermectin — a generic medication that doctors had success treating COVID-19 with early on — was quickly vilified, as were the doctors who attempted to prescribe it for COVID-19 patients.
In his book, “The War on Ivermectin: The Medicine That Saved Millions and Could Have Ended the COVID Pandemic,” Dr. Pierre Kory details Big Pharma’s suppression of this drug when it was found to work against COVID-19. When he and colleagues first spoke out about the drug’s potential, however, he was naïve. He said during our 2022 interview:15
“I worked a lot and I got deeply expert on ivermectin. But what happened in the next few months is that everything started going sideways, and I could not figure it out. I saw hit pieces … The thing is, I didn’t know. I didn’t know that what I was really doing — bringing forth data supporting the efficacy of a generic drug — that is poking the bear.
And when I say poking the bear, what is anathema to the pharmaceutical industry and their whole business model is they cannot have generic off-patent drugs become standard of care. It obliterates the market for their pricing new pills.
I didn’t know I was stepping into a war. In the history of pharma, I don’t think any single medicine threatened as many [drug] markets and campaigns. The only other medicine that did that was hydroxychloroquine, but they already killed hydroxychloroquine in 2020.
I was coming out now with ivermectin, and it threatened hundreds of billions of dollars in perpetuity for these insanely lethal vaccines, monoclonal antibodies, remdesivir, paxlovid, molnupiravir — all of the markets for their novel new pills to enter. I mean, I don’t think any medicine has ever threatened that much of a market.”
‘A Problem for Many Reasons’
If the FDA is allowed to ban medications for certain uses, we’ll see more of what happened with ivermectin. It’s a “problem for many reasons,” Zinberg explains:16
“The statute gives the FDA the power, without any public input, to prevent patients’ access to off-label therapies even though their physicians and their patients have found the treatments to be beneficial or even essential.
… Allowing the FDA to ban certain off-label uses will impair clinical progress. Off-label use enables physicians to assess their patients’ unique circumstances and use their own evolving scientific knowledge in deciding to try approved products for new indications.
If the treatment proves useful, formal studies are performed and published. If enough evidence accumulates, the treatment becomes the standard of care, even if the manufacturer didn’t submit the product for a separate, lengthy and costly FDA review.
… Substituting regulators’ wisdom for the cost-benefit judgment of physicians and their patients will discourage attempts to use approved products in new and beneficial ways and deprive patients of valuable treatments. Congress should reconsider this ill-advised legislation.”
California Law Also Shackles Doctors’ Freedoms
In California, regulators are also interfering with the practice of medicine. Law AB 2098, which was signed into law September 30, 202217 and went into effect January 1, 2023,18 gives the state power to take away doctors’ medical licenses if they spread “misinformation” that goes against the standard COVID-19 rhetoric.
Specifically, those who “disseminate or promote misinformation or disinformation related to COVID-19, including false or misleading information regarding the nature and risks of the virus, its prevention and treatment; and the development, safety, and effectiveness of COVID-19 vaccines” could be “disciplined,” which includes loss of their medical license.19
It’s akin to putting shackles on their wrists, forcing them to conform to a narrative intent on pushing dangerous gene therapies and ineffective medications. It’s also a potential warning of darker things to come.
What constitutes “misinformation” or “disinformation” worthy of taking away a person’s medical license? It’s anyone’s guess, really, but doctors afraid of being punished are likely to steer clear of anything that could possibly fit under this definition — to the detriment of their patients.
Bill 2098 itself is packed with misinformation and ignores the scientific truths about COVID-19,20 such as the fact that prior infection with COVID-19 results in natural immunity — immunity that’s superior to that achieved via a COVID-19 shot.21
The bill, if it passes, will stop doctors from practicing medicine the way they deem best for the individual patient. It will also stop dissent — even when dissent is necessary and beneficial, and coming from people with expertise. And that’s precisely the point.22 In December 2022, Physicians for Informed Consent sued the state of California, arguing that AB 2098 violates the U.S. Constitution.
According to a news release, “The lawsuit argues that the State has weaponized the vague phrase ‘misinformation,’ thereby unconstitutionally targeting physicians who publicly disagree with the government’s public health edicts on COVID-19.”23
This Shift Isn’t Just for the US
It’s important to note that the trend to let a Pharma-controlled government silence your doctor and dictate basic components of your medical care is not confined to the U.S. — it’s happening globally.
Proposed amendments to the 2005 International Health Regulations (IHR), for instance, aim to erase the concepts of human dignity, human rights and fundamental freedoms from the equation.24 The first principle in Article 3 of the 2005 IHR states that health regulations shall be implemented “with full respect for the dignity, human rights and fundamental freedoms of persons.” The amendment strikes that sentence.
Instead, international health regulations will be based on “principles of equity, inclusivity and coherence” only. This means they can force you to undergo whatever medical intervention they deem to be in the best interest of the collective.
Individuals won’t matter. Human dignity will not be taken into consideration. Human rights will not be taken into consideration, and neither will the concept that human beings have fundamental freedoms that cannot be infringed. Autonomy over your body will be eliminated. You’ll have no right to make personal health decisions.
While it may start slowly, such as with Pharma’s quiet move to ban off-label usage of medications for certain uses, it will soon expand, chipping away at your sovereignty until it’s gone. This is why it’s imperative to share this knowledge and support measures that protect our human rights and individual freedoms.
Dr. Suneel Dhand 280K subscribers 44,354 views Oct 18, 2022I will not be joining any of these again or attending their conferences. Join my Red-Pilled Community and Follow me on Locals, the uncensored platform, for more open and real discussions: https://drsuneeldhand.locals.com Subscribe to my Newsletter here: https://suneeldhand.com/newsletter/
Over 5,200 physicians and medical scientists worldwide have signed the “Rome Declaration” to alert citizens about the deadly consequences of Covid-19 policy makers’ and medical authorities’ unprecedented behavior; behavior such as denying patient access to lifesaving early treatments, disrupting the sacred, physician-patient relationship and suppressing open scientific discussion for profits and power.
The Declaration was created by physicians and scientists during the Rome Covid Summit, and immediately catalyzed support from doctors around the world. These professionals, many of whom are on the front lines of pandemic treatment, have experienced career threats, character assassination, censorship of scientific papers and research, social media accounts blocked, online search results manipulated, clinical trials and patient observations banned, and their professional history and accomplishments minimized in both academic and mainstream media.
Though the declaration’s signatories are diverse in their specialties, treatment philosophies and medical opinions, they have risen up to take a collective stand against authoritarian measures by corporations, medical associations, and governments and their respective agencies. The objective of the declaration is to reclaim their leadership role in conquering this pandemic.
In concert with the declaration, the signatories have created a “Doctors – and Scientists-only” COVID information platform so that citizens can make informed decisions for their families without interruption, manipulation, politicization, or profiteering from external forces outside of the doctor-patient relationship.
Dr. Robert Malone, architect of the mRNA vaccine platform, reads the Rome Declaration (video):
Many of you are looking for and sharing the website for the NZ Doctors Speaking Out With Science (NZDSOS). Tonight someone has sent me a fraudulent website set up to clearly confuse people and sabotage the work of this organisation of brave Doctors willing to stand up and demand Informed Consent for New Zealanders. Please be very careful to use the CORRECT web address for NZDSOS, instead of this troublesome one.
Jummai Nache Pfizer 1st February 2021 Severe Adverse Reaction: Amputation of both legs and more recently both hands, blood clots, Cardiomyopathy and more.
Philip Telling the Story of his Wife Jummai This is the story about my wife Jummai. She is a medical assistant who worked in one of the clinics in Minneapolis MN, where she was instructed to take the Covid-19 vaccine. After receiving her second Pfizer Covid-19 vaccine on 1st February 2021 she started to experience chest pain at work. Three days after the chest pains I took her to Urgent Care on February 6, 2021. After the checkup, EKG and other tests, the doctor said there was nothing wrong with her chest and every test showed she was okay. She took a covid-19 test and the next day was confirmed positive. Jummai and I were shocked when we received the result that she was covid-19 positive because she had not manifested any symptom before taking the shot. But we later accepted that perhaps, the virus and the vaccine together contributed to the adverse reaction on her body based on the report of the Infectious Disease physician that Jummai was asymptomatic. So Jummai followed the CDC guidelines but then a few days later she ended up at Fairview ER and then was transferred to U of M medical center. The next day, 2/14/21 the doctor called and told me that her heart was deteriorating, her oxygen levels and blood pressure were low and she needed to be put on a ventilator. I gave approval for them to proceed with the ventilator as needed.
Jummai Nache with legs amputated following the Pfizer mRNA vaccine
The Infectious Disease Dr considered the test results, Jummai’s condition, the timeline of the administered vaccine and the onset of covid 19, realizing the vaccine might have caused the adverse reaction. But the Dr always concludes that this is just a theory which cannot be verified because they do not have testing equipment to clearly state that the vaccine has caused Jummai’s devastation. Whatever the cause may be, my wife is suffering unbearable excruciating pain and permanent catastrophic damage. The consequences of the adverse event are as follows:
Arterial blood clot;
Respiratory distress—ventilator;
Cardiomyopathy;
Anemia;
Damage to fingers of both hands and toes of both feet;
Ischemia;
MIS-Multiple Inflammatory Syndrome.
Amputation of Both Legs and Hands As a result of the above complications, the Infectious Disease Dr decided to forward the case to CDC. According to the Dr, after going back and forth with the CDC, they decided to meet to deliberate with many experts around the country in which about 70-80 doctors met on a virtual call to discuss Jummai’s case. About 8 weeks after the meeting the CDC sent us a letter of their conclusions which stated that Jummai was infected with MIS-A and covid-19, but they cannot conclude whether the covid-19 vaccine contributed for now. On one occasion, the doctor called and told me that Jummai could die at any moment, but God preserved my wife’s life in a miraculous way in response to all the prayers of the church. He has continued to do amazing things in her life, to which we testify. Three weeks ago, the cardiologist told us that Jummai’s heart is 100% healed. By God’s grace, this goes against the initial report which was that her heart would never be the same. To God be the glory! I have also appreciated God’s grace of healing her from the life-threatening impact of the vaccine/Covid-19 destruction, but it has required high risk surgeries for amputation of both legs (below the knees). When those are healed, she is yet to undergo amputations at both hands. My experience on this journey has been so difficult but I can’t imagine the excruciating pain mentally, physically and emotionally that my wife is going through. I can only equate her experience and challenge with Job’s experience and trial in the sense that the challenges have come in degrees, one after another. She would have one challenge and we would thank God as overcomers and then the devil would present the next challenge and we would overcome yet again. Time and again, challenge after challenge.
The following is the text of the open letter written by Dr. Tess Lawrie to Dr. June Raine, chief executive of the UK’s Medicines and Health Care Regulatory Agency (MHRA) demanding the halt of the mass rollout of COVID vaccines after discovering a “high number of COVID-19 vaccine-attributed deaths and ADRs [adverse drug reactions] that have been reported via the Yellow Card system”. The Yellow Card review includes reports from January 4, 2021 to May 26, 2021.
Dr. Lawrie goes on to summarize the findings of their rapid report on ADRs. Here are some of them:
“sudden death” of 438 people following vaccination;
152 fatalities from brain bleeds and clots;
103 fatalities from pulmonary embolism;
and 81 due to cardiac categories;
13,766 bleeding, clotting and ischaemic ADRs were identified;
54, 870 ADRs and 171 fatalities due to immune system disorders
Some people who experienced “infection” ADRs were cases of re-activated latent viruses, including Herpes Zoster or shingles (1,827 ADRs), Herpes Simplex (943 ADRs, 1 fatal), and Rabies (1 fatal ADR).
157,579 people experienced pain after vaccination
185,474 or 21% of all ADRs were categorized as nervous system disorders. A variety of neurological disorders were noted, including paralysis, palsy, Guillain-Barre, multiple sclerosis, neurodegeneration, seizure, among others.
4,771 people experienced visual impairments including blindness
Dr. Lawrie says that their preliminary review suggests that the ADRs they found was not limited to any one vaccine (all vaccines were causing ADRs).
The open letter goes on to say: “The nature and variety of ADRs reported to the Yellow Card System are consistent with the potential pathologies described in this paper and supported by other recent scientific papers on vaccine-induced harms, which are mediated through the vaccine spike protein product. It is now apparent that these products in the blood stream are toxic to humans. An immediate halt to the vaccination programme is required whilst a full and independent safety analysis is undertaken to investigate the full extent of the harms.”
Editor’s Note: Governments have been said that their implementation of lockdowns, masks, physical distancing, and now, universal vaccination, are precautionary measures to prevent the devastation of societies. It then follows that if governments were truly protecting societies, then they know that the most prudent approach is to suspend all vaccination campaigns.
Governments and their regulatory agencies knew from the beginning that all these vaccines were experimental products. As such, careful collection of data is a must. Now that the data for millions of vaccine recipients is here, and hundreds of thousands of vaccine injuries are appearing, it is time for governments to accept that these vaccines are dangerous and must be stopped [see New study: Vaccines are the likely cause of adverse effects and deaths following vaccination].
I rather wonder at all these so called ‘slips’ … are they merely laughing at us. There have been so many of these now, even from a vaccine ‘expert’ here in NZ. (She is on video on the news page, right column).
Here are the links to these latest ones (be aware the twitter one may well disappear):
Five times more children and young people committed suicide than died of COVID-19 during the first year of the pandemic in the United Kingdom, according to a study, which also concluded that lockdowns are more detrimental to children’s health than the virus itself.
Greece has become the latest European country to be hit with mass protests after the government announced the unvaccinated would be banned from visiting bars, restaurants, cinemas and other public places.
Thousands of demonstrators descended on Athens and Thessaloniki, with crowds chanting “Hands off our kids!” and holding signs that said “We say no to vaccine poison.”
All nursing home staff and hospital workers will be mandated to get the vaccine from August 16, while hospital workers also face losing their jobs unless they get the compulsory jab from September.
World wide the call has been to send teams door to door (in some places accompanied by the military or the Police) to administer the CV VX.
The Whanganui DHB is ‘getting the vx to the vulnerable’ by sending a team of two to your door. The ‘disabled, frail or elderly’ who can’t make it to the clinic. The team will be increased to four in August and so far 20,000 doses have been delivered in the Whanganui area.
Should you be unaware of the list of full, possible side effects provided by the FDA, which note, exceed considerably the list provided on the NZ health website see details below.
Here are those supplied by the authorities in NZ:
The most common reported reactions are:
pain or swelling at the injection site
feeling tired or fatigued
headache
muscle aches
chills
joint pain
fever
redness at the injection site
nausea.
Uncommon side effects
In the clinical trials, uncommon side effects were reported in every 1 in 100 to 1 in 1,000 people. These include:
You aren’t necessarily going to get all of those or even any of them if you have the vaccine. But those are the possible side effects that the FDA has listed. They’re all unpleasant, most of them very serious and you can’t get more serious than death. Below are the deaths & injuries reported to the official government data bases that occurred after taking the covid-19 injection. Remember only 1% on average are reporting.
CURRENT DEATH & INJURY STATS REPORTED:
USA: DEATHS – 9,048 INJURIES: 520,747 (to July 2 )
UK: 1,403 DEATHS – INJURIES 1,007,253 (to June 23)
EUROPE: 17,503 – INJURIES 1,687,527 (to July 3)
AUSTRALIA – 313 DEATHS – 24000 INJURIES (to 20 June)
For the articles on the deaths and injuries cited, go to the news page and at the right hand column, click on the images stating the stats.
AMAZING conversation! Four physicians from across Canada, along with a legal representative for their separate cases, tell their stories of persecution at the hands of their governing bodies. Their only crime – practicing evidence-based medicine by questioning the safety of their patients and the public during the pandemic. These physicians, and others like them, are the living embodiment of the medical mantras of “do no harm” and “informed consent”.
[NOTE: The last twelve minutes of this video consist of an audio recording alone and has no video component.] While it survives at YT: https://www.youtube.com/watch?v=GpViJcdJFkc
KHUSHAB, PUNJAB — A police superintendent is dead in what may be the fastest death we’ve covered on this blog.
Mr. Malik Imtiaz Mahmood was the Superintendent of Police for the city of Khushab. He received his experimental injection against COVID-19 on or around June 13, according to the World Doctors Alliance. The organization shared a photo of Mr. Mahmood receiving the injection.
Read more below (video included as the superintendent collapses):
While the list of crimes committed by authorities during the COVID-19 pandemic is a long one, perhaps the biggest crime of all is the purposeful suppression of safe and effective treatments, including ivermectin. This appears to have been done to protect the COVID “vaccine” program
The COVID shots were brought to market under emergency use authorization (EUA), which can only be obtained if there are no other safe and effective alternatives available
Several systematic reviews and meta-analyses of studies looked at ivermectin for the prevention and treatment of COVID-19 infection. A rapid review performed on behalf of the Front Line COVID-19 Critical Care Alliance (FLCCC) in the U.S., January 3, 2021, found the drug “probably reduces deaths by an average 83% compared to no ivermectin treatment”
According to a more recent review and meta-analysis, ivermectin, when used preventatively, reduced COVID-19 infection by an average 86%
Another recent scientific review concluded ivermectin produces large statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance
While the list of crimes committed by authorities during the COVID-19 pandemic is a long one, perhaps the biggest crime of all is the purposeful suppression of safe and effective treatments. At this point, it seems quite clear that this was done to protect the COVID jab rollout.
The COVID shots were brought to market under emergency use authorization (EUA), which can only be obtained if there are no other alternatives available. In a sane world, the COVID gene therapies would never have gotten an EUA, as there are several safe and effective treatment options available.
One treatment that stands out above the others is ivermectin, a decades-old antiparasitic drug that is on the World Health Organization’s list of essential medications.
What makes ivermectin particularly useful in COVID-19 is the fact that it works both in the initial viral phase of the illness, when antivirals are required, as well as the inflammatory stage, when the viral load drops off and anti-inflammatories become necessary. It’s been shown to significantly inhibit SARS-CoV-2 replication in vitro,1 speed up viral clearance and dramatically reduce the risk of death.
Gold Standard Review Supports Use of Ivermectin
Dr. Tess Lawrie, a medical doctor, Ph.D., researcher and director of Evidence-Based Medicine Consultancy Ltd (video above).2 in the U.K., has been trying to get the word out about ivermectin. To that end, she helped organize the British Ivermectin Recommendation Development (BIRD) panel3 and the International Ivermectin for COVID Conference,4 which was held online, April 24, 2021.
Twelve medical experts5 from around the world shared their knowledge during this conference, reviewing mechanism of action, protocols for prevention and treatment, including so-called long-hauler syndrome, research findings and real world data. All of the lectures, which were recorded via Zoom, can be viewed on Bird-Group.org.6
Lawrie has published several systematic reviews and meta-analyses of studies looking at ivermectin for the prevention and treatment of COVID-19 infection. A rapid review performed on behalf of the Front Line COVID-19 Critical Care Alliance (FLCCC) in the U.S., January 3, 2021, found the drug “probably reduces deaths by an average 83% compared to no ivermectin treatment.”7
Her February 2021 meta-analysis, which included 13 studies, found a 68% reduction in deaths. This is an underestimation of the beneficial effect, because one of the studies included used hydroxychloroquine (HCQ) in the control arm. Since HCQ is an active treatment that has also been shown to have a positive impact on outcomes, it’s not surprising that this particular study did not rate ivermectin as better than the control treatment (which was HCQ).
Two months later, March 31, 2021, Lawrie published an updated analysis that included two additional randomized controlled trials. This time, the mortality reduction was 62%. When four studies with high risk of bias were removed during a subsequent sensitivity analysis, they ended up with a 72% reduction in deaths.
(Sensitivity analyses are done to double-check and verify results. Since the sensitivity analysis rendered an even better result, it confirms the initial finding. In other words, ivermectin is unlikely to reduce mortality by anything less than 62%.)
Lawrie reviewed the February and March analyses and other meta-analyses in an interview with Dr. John Campbell, featured in “More Good News on Ivermectin.” Lawrie has now published her third systematic review. According to this paper, published June 17, 2021 in the American Journal of Therapeutics:8
“Meta-analysis of 15 trials found that ivermectin reduced risk of death compared to no ivermectin (average risk ratio 0.38 …) … Low-certainty evidence found that ivermectin prophylaxis reduced COVID-19 infection by an average 86% … Secondary outcomes provided less certain evidence.
Low-certainly evidence suggested that there may be no benefit with ivermectin for ‘need for mechanical ventilation,’ whereas effect estimates for ‘improvement’ and ‘deterioration’ clearly favored ivermectin use. Severe adverse events were rare among treatment trials …”
World Health Organization Refuses to Recommend Ivermectin
Despite the fact that most of the evidence favors ivermectin, when the WHO finally updated its guidance on ivermectin at the end of March 2021,9,10 they largely rejected it, saying more data are needed. They only recommend it for patients who are enrolled in a clinical trial.
Yet, they based their negative recommendation on a review that included just five studies, which still ended up showing a 72% reduction in deaths. What’s more, in the WHO’s summary of findings, they suddenly include data from seven studies, which combined show an 81% reduction in deaths. The confidence interval is also surprisingly high, with a 64% reduction in deaths on the low end, and 91% on the high end.
Even more remarkable, their absolute effect estimate for standard of care is 70 deaths per 1,000, compared to just 14 deaths per 1,000 when treating with ivermectin. That’s a reduction in deaths of 56 per 1,000 when using the drug. The confidence interval is between 44 and 63 fewer deaths per 1,000.
Despite that, the WHO refuses to recommend this drug for COVID-19. Rabindra Abeyasinghe, a WHO representative to the Philippines, commented that using ivermectin without “strong” evidence is “harmful” because it can give “false confidence” to the public.11
Why Ivermectin Has Been Censored
If you’ve been trying to share the good news about ivermectin, you’re undoubtedly noticed that doing so is incredibly difficult. Many social media companies are banning such posts outright.
Promoting ivermectin on YouTube, or even discussing benefits cited in published research, violates the platform’s posting policies. DarkHorse podcast host Bret Weinstein, Ph.D., is but one of the victims of this censorship policy.
His interviews with medical and scientific experts such as Dr. Pierre Kory, a lung and ICU specialist, former professor of medicine at St. Luke’s Aurora Medical Center in Milwaukee, Wisconsin, and the president and chief medical officer12 of the FLCCC, and Dr. Robert Malone, the inventor of the mRNA and DNA vaccine core platform technology,13 have been deleted from the platform. The interview with Malone had more than 587,330 views by the time it was wiped from YouTube.14
But why? Why don’t they want people to feel confident that there’s treatment out there and that COVID-19 is not the death sentence they’ve been led to believe it is? The short answer is because ivermectin threatens the vaccine program. As explained by Andrew Bannister in a May 12, 2021, Biz News article:15
“What if there was a cheap drug, so old its patent had expired, so safe that it’s on the WHO’s lists of Essential and Children’s Medicines, and used in mass drug administration rollouts?
What if it can be taken at home with the first signs COVID symptoms, given to those in close contact, and significantly reduce COVID disease progression and cases, and far fewer few people would need hospitalization?
The international vaccine rollout under Emergency Use Authorization (EUA) would legally have to be halted. For an EUA to be legal, ‘there must be no adequate, approved and available alternative to the candidate product for diagnosing, preventing or treating the disease or condition.’
The vaccines would only become legal once they passed level 4 trials and that certainly won’t happen in 2021 … The vaccine rollout, outside of trials, would become illegal.
The vaccine manufactures, having spent hundreds of million dollars developing and testing vaccines during a pandemic, would not see the $100bn they were expecting in 2021 … Allowing any existing drug, at this time, well into stage 3 trials, to challenge the legality of the EUA of vaccines, is not going to happen easily.”
The WHO and Drug Companies Are Severely Compromised
The WHO’s rejection of ivermectin only makes sense if a) you take into account the EUA requirements; and b) remember that the WHO receives a significant portion of its funding from private vaccine interests.
The Bill & Melinda Gates Foundation is the second largest funder of the WHO after the United States, and The GAVI Alliance, also owned by Gates, is the fourth largest donor. The GAVI Alliance exists solely to promote and profit from vaccines, and for several years, the WHO director-general, Tedros Adhanom Ghebreyesus, served on the GAVI board of directors.16
As reported by Bannister, Merck, the original patent holder of ivermectin, also has severe conflicts of interest that appear to have played a role in the rejection of ivermectin. He writes:17
“Ivermectin has been used in humans for 35 years and over 4 billion doses have been administered. Merck, the original patent holder,18 donated 3.7 billion doses to developing countries … Its safety is documented at doses twenty times the normal …
Merck’s patent on Ivermectin expired in 1996 and they produce less than 5% of global supply. In 2020 they were asked to assist in Nigerian and Japanese trials but declined both.
In 2021 Merck released a statement claiming that Ivermectin was not an effective treatment against Covid-19 and bizarrely claimed, ‘A concerning lack of safety data in the majority of studies’ of the drug they donated to be distributed in mass rollouts, by primary care workers, in mass campaigns, to millions in developing countries.
The media reported the Merck statement as a blinding truth without looking at the conflict of interests when days later, Merck received $356m from the US government to develop an investigational therapeutic.
The WHO even quoted Merck, as evidence, that it didn’t work, in their recommendation against the use of Ivermectin. It’s a dangerous world when corporate marketing determines public health policy.”
FLCCC Calls for Widespread and Early Use of Ivermectin
In the U.S., the FLCCC has been calling for widespread adoption of ivermectin, both as a prophylactic and for the treatment of all phases of COVID-19,19,20 and Kory has testified to the benefits of ivermectin before a number of COVID-19 panels, including the Senate Committee on Homeland Security and Governmental Affairs in December 202021 and the National Institutes of Health COVID-19 Treatment Guidelines Panel in January 2021.22
Based on a meta-analysis of 18 randomized controlled trials, ivermectin produces large statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance.
As noted by the FLCCC:23
“The data shows the ability of the drug Ivermectin to prevent COVID-19, to keep those with early symptoms from progressing to the hyper-inflammatory phase of the disease, and even to help critically ill patients recover.
… numerous clinical studies — including peer-reviewed randomized controlled trials — showed large magnitude benefits of Ivermectin in prophylaxis, early treatment and also in late-stage disease. Taken together … dozens of clinical trials that have now emerged from around the world are substantial enough to reliably assess clinical efficacy.”
The FLCCC has published three different COVID-19 protocols, all of which include the use of ivermectin:
I-MASK+24 — a prevention and early at-home treatment protocol
I-MATH+25 — an in-hospital treatment protocol. The clinical and scientific rationale for this protocol has been peer-reviewed and was published in the Journal of Intensive Care Medicine26 in mid-December 2020
I-RECOVER27 — a long-term management protocol for long-haul syndrome
In addition to Lawrie’s meta-analysis in the American Journal of Therapeutics, the FLCCC has also published a scientific review28 in that same journal.
This paper, “Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19,” published in the May/June 2021 issue, found that, based on a meta-analysis of 18 randomized controlled trials, ivermectin produces “large statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance.”
Ivermectin Significantly Reduces Infection Risk and Death
The FLCCC also found that when used as a preventive, ivermectin “significantly reduced risks of contracting COVID-19.” In one study, of those given a dose of 0.4 mg per kilo on Day 1 and a second dose on Day 7, only 2% tested positive for SARS-CoV-2, compared to 10% of controls who did not get the drug.
In another, family members of patients who had tested positive were given two doses of 0.25 mg/kg, 72 hours apart. At follow up two weeks later, only 7.4% of the exposed family members who took ivermectin tested positive, compared to 58.4% of those who did not take ivermectin.
In a third, which unfortunately was unblended, the difference between the two groups was even greater. Only 6.7% of the ivermectin group tested positive compared to 73.3% of controls. According to the FLCCC, “the difference between the two groups was so large and similar to the other prophylaxis trial results that confounders alone are unlikely to explain such a result.”
The FLCCC also points out that ivermectin distribution campaigns have resulted in “rapid population-wide decreases in morbidity and mortality,” which indicate that ivermectin is “effective in all phases of COVID-19.” For example, in Brazil, three regions distributed ivermectin to its residents, while at least six others did not. The difference in average weekly deaths is stark.
In Santa Catarina, average weekly deaths declined by 36% after two weeks of ivermectin distribution, whereas two neighboring regions in the South saw declines of just 3% and 5%. Amapa in the North saw a 75% decline, while the Amazonas had a 42% decline and Para saw an increase of 13%.
It’s worth noting that ivermectin’s effectiveness appears largely unaffected by variants, meaning it has worked on any and all variants that have so far popped up around the world. Additional evidence for ivermectin will hopefully come from the British PRINCIPLE trial,29 which began June 23, 2021. Ivermectin will be evaluated as an outpatient treatment in this study, which will be the largest clinical trial to date.
Ivermectin in the Treatment of Long-Haul Syndrome
The FLCCC believes ivermectin may also be an important treatment adjunct for long-haul COVID syndrome. In their June 16, 2021, video update, the team reviewed the newly released I-RECOVER protocol.
Keep in mind that ivermectin is not to be used in isolation. Corticosteroids, for example, are often a crucial treatment component when organizing pneumonia-related lung damage is present. Vitamin C is also important to combat inflammation. Be sure to work with your doctor to identify the right combination of drugs and supplements for you.
Last but not least, as noted by Kory in this video, it’s really important to realize that long-haul syndrome is entirely preventable. The key is early treatment when you develop symptoms of COVID-19.
While ivermectin has a good track record when it comes to prevention and early treatment, it can be tricky to obtain, depending on where you live and who your doctor is.
A highly effective alternative that anyone can use, anywhere, is nebulized hydrogen peroxide. It’s extremely safe and very inexpensive. The biggest cost is the one-time purchase of a good tabletop jet nebulizer. To learn more, download Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery,” in which he details how to use this treatment.
After being in the “hesitant” category for several months I am now in the “no” category. As a retired medical doctor I have plenty of time, and a genuine fascination, to thoroughly research this topic. I have been diligently reviewing every scientific journal I can find, reading every online news article I come across, and going through countless case reports on the CDC VAERS website. I now have a clearer understanding of how these vaccines influence our immune system and organs, how they could be of benefit, and how they cause the multiple short, medium, and long term adverse effects.
I am convinced that the benefits promoted by experts on TV regarding these vaccines are less than what they promise, and the adverse reactions are more than they want us to believe. The effects of these vaccines on the human body are infinetely more complex than anyone can imagine… a million shades of gray, you may say.
Evidence suggests people who have received the COVID “vaccine” may have a reduced lifespan as a result of the acute, subacute and long-term effects from the COVID injection
If you’ve gotten the COVID shot, consider yourself high risk for COVID and implement a daily prophylaxis protocol. This means optimizing your metabolic flexibility, vitamin D, and taking vitamin C, zinc and a zinc ionophore on a daily basis, at least throughout cold and flu season
Evidence shows NAC may be used to prevent blood clots and break up any that might already have formed
If you’re low risk for COVID and have not been vaccinated, make sure you have these items on hand and begin treating at the very first signs of cold or flu symptoms
Also buy yourself a tabletop jet nebulizer, some saline solution and food grade hydrogen peroxide. Nebulized peroxide is an excellent go-to both for prevention and treatment, regardless of the stage the respiratory infection is in. For prevention, nebulize every other day. For treatment, use at first signs of respiratory infection
In this interview, return guest Dr. Vladimir Zelenko discusses an incredibly serious concern, one shared with at least two other highly credible experts — Michael Yeadon, Ph.D., a life science researcher and former vice-president and chief scientist of allergy and respiratory research at Pfizer, and professor Luc Montagnier, a world-renowned virologist who won the Nobel prize for his discovery of HIV.
Yeadon, Montagnier and Zelenko all believe the COVID-19 shots could reduce life expectancy by several decades, depending on several factors, including whether you’re required to get booster shots. In fact, there may be reason to suspect that many who get the jabs and subsequent boosters could lose their lives within two to three years, as a result of pathogenic priming.1,2
Many may not realize that when I was a youngster I was a Boy Scout, but you might know their motto is “Be Prepared.” It is an approach that has served me well over the years. I am not stating unequivocally that dire outcome will materialize, as my interview next week with Dr. Peter McCullough goes into. However, it would seem prudent to have a good protocol in your hands in anticipation of a worst-case scenario.
So, on that note, Zelenko and I take a deep dive into what can be done to prevent such a fate. Zelenko categorizes the risks of COVID-19 “vaccines” into three categories: acute, subacute and long-term, so let’s begin by reviewing the primary risks found in each of these categories.
Risk Category No. 1 — Acute Risks
The acute phase of harm begins at the moment of injection and likely lasts for about three months or so. Based on reports filed with the U.S. Vaccine Adverse Event Reporting System (VAERS), it’s clear that many cannot survive past the acute phase.
About 6,000 deaths have been reported so far, and death commonly occurs within 48 hours of injection. Many serious disabling events also occur rather rapidly, typically within a few days or weeks. However, Zelenko has a very dismal perspective on the accuracy of the VAERS database. He explains:
“According to a paper published by the Salk Institute in San Diego, they’ve discovered that the spike protein that’s generated through the vaccination itself has negative health effects. It’s toxic … on its own …
There’s plenty of evidence that shows that it spreads from the injection site and goes to the bloodstream, and basically comes into every single cell in the body.3,4
mRNA has a half-life of around one to two weeks, depending on the mRNA, and during that interim, each mRNA molecule makes around 2,000 to 5,000 spike proteins. So, we’re talking about trillions and trillions of spike proteins.
Your entire body becomes a spike protein factory. Several orders of magnitude more than if you were to get COVID, because COVID infects the upper and lower airways primarily. Those are the cells that get infected and begin to produce spike proteins. But here we’re injecting the vaccine and it actually travels to every single cell in your body and converts every single cell in your body into a factory for spike proteins.”
As the mRNA disseminates through your vascular system, the cells lining your blood vessels begin producing spike protein. This is why we’re seeing such a staggering number of reports of people experiencing blood clots from these injections.
According to Zelenko, 40% of these events occur within the first two days after injection. The risk then diminishes, but vascular events such as heart attacks, strokes, renal infarcts and pulmonary infarcts don’t completely peter out until about three months after the last injection.
But these events of the past three months are not being reported to VAERS. It is, of course, possible that people simply aren’t connecting them to the COVID shot they got several months earlier.
How Many Have Actually Died From the COVID Shots?
As noted by Zelenko, underreporting is part of the problem we’re facing. The real number of side effects is impossible to determine, given the fact that the Food and Drug Administration didn’t insist on a robust post-vaccination data collection system, but it’s most certainly higher than what VAERS is listing.
“If you look at the VAERS [vaccine adverse event reporting system], which in my opinion is a piece of garbage … as of today, let’s say says there’s 6,000 deaths associated with taking the vaccine. Well, we need to understand what that actually means,” Zelenko says.
“If you look at the 2009 Harvard study on the VAERS system, they said only 1% of events are actually reported. So, OK … whatever the number is, it’s not 6,000. Maybe only 10% are being reported. I don’t know. But definitely it’s being underreported.
And then there’s two [additional] big problems. There’s evidence coming out that VAERS reports that have been filed are being erased off the server, No. 1. No. 2, I personally know of two dozen cases of deaths associated with the vaccine, and the doctor and/or family members that tried to file a VAERS report, their reports were rejected due to some technicality.
The fact that they all couldn’t make a report, that raises my eyebrows. What percentage of the information are we actually seeing? The answer is, I estimate, there are already around 200,000 dead Americans, directly related to the vaccinations.”
To get to that number, Zelenko assumes only 10%5 of adverse effects are reported. Studies have indicated it could be as low as 1%.6,7 That gives us a death toll of about 60,000, to which he adds another 140,000 given the fact that reports are being scrubbed and refused.
“The point is that it should definitely raise eyebrows and have the public start screaming and saying, ‘We want to know the truth. We want to know the accurate numbers. Stop suppressing the truth … I want to be able to make an informed choice whether or not I want to take this injection.’ And that’s not being given to the people.
My problem is not with the vaccine. My problem is with the government, governing bodies and certain people that are obstructing the flow of life saving information and suppressing the truth from people, and then using coercion to force people to take this vaccine. That’s the nefarious part.
The suppression is so blatant and so overt that doctors with impeccable credentials are being deplatformed for just voicing an opinion. And then you couple that together with proven prehospital treatment approaches and protocols that have been proven to reduce hospitalization and death by 85%, and that information is being suppressed.
So here you have a dual censorship where the positive, hopeful, life-saving information is being suppressed and the dangerous outcomes of the vaccination approach is being suppressed. It’s a perfect setup for genocide.”
Risk Category No. 2 — Subacute Risks
The subacute risk phase, which begins around three months’ post-injection, is exceedingly difficult to quantify. At bare minimum, it’s likely to last several months to a couple of years. The primary concern now is antibody-dependent enhancement (ADE), also referred to as pathogenic priming and/or paradoxical immune enhancement (PIE) as it more accurately describes the disease mechanism.
Zelenko believes the mRNA will have degraded by this time, and your cells will hopefully no longer produce spike protein. I believe he may be overly optimistic here, as the synthetic mRNA has been genetically modified to be less perishable, plus it’s encased in a nanolipid to resist breakdown.
I suspect this modified mRNA may remain viable far longer than anyone suspects, thanks to its synthetic nature. What’s more, there’s a mechanism by which the mRNA can be reverse transcribed into your DNA, which would make the spike protein production permanent — and probably intergenerational. I describe this process in “The Many Ways in Which COVID Vaccines May Harm Your Health.”
If Zelenko is correct, then the primary disease agent now switches from the spike protein to the antibodies produced in response to the spike protein. We don’t know how long these antibodies will last, but chances are they’ll stick around for a number of months or years.
While antibody production is the primary purpose of these shots, and the response said to provide you an immune benefit, they can actually be the source of problems.
Animal trials in which conventional coronavirus vaccines were tested have shown coronavirus vaccines routinely cause ADE,8,9,10,11,12 so when the animals are challenged with the real virus they’ve been immunized against, they can get seriously ill and even die. If hospitals start filling up with vaccinated individuals this fall, you’ll know why. They’re suffering the effects of ADE.
“In other words, those antibodies that were produced with the vaccination were pathologic,” Zelenko says. “They were lethal and they led to an exaggerated immune response. That’s what it means, antibody-dependent enhancement. It’s an enhancement of your immune response in a way that it will kill you …
The question is, how safe is it long-term, or in the subacute [phase] from three months to three years? That is a big question mark. Based on animal models — and this is what Dr. Mike Yeadon is saying — it could be absolutely genocidal. It’s the biggest gamble on the survival of humanity in the history of humanity.”
However, as a counter to this view, Dr. Peter McCullough, who is in complete agreement with the engineering of this event and it being one of the most egregious crimes against humanity, is not convinced that there will be a massive die-off in the fall.
He is well-trained in the science and has essentially completed a fellowship in COVID-19 along with being the senior editor of two prestigious medical journals so his opinion also deserves consideration. We will be posting his interview next Sunday, July 11, 2021.
Why Is Humanity’s Survival Being Risked?
The questions on many people’s mind right now are, “Why are lifesaving early treatment approaches suppressed?” “Why are the toxic side effects and death rates of the vaccines being suppressed?” and “Why are entire continents being coerced into taking a vaccine that is both medically unnecessary and unproven in terms of safety and effectiveness?”
Taken together, none of it makes any sense, which is why people like Yeadon, Montagnier, Zelenko and others are raising concerns about global genocide. Is that what this is all about? Is there an alternative interpretation of what’s happening? When you consider the actual data, mass vaccination simply isn’t necessary, so why the frantic push to get a needle in every arm? Zelenko explains:
“There’s something called medical necessity. So, let’s analyze if there’s any medical necessity for this vaccine, and you have to do that in a systematic way based on demographics.
If you look at the CDC’s data, anyone 18 and younger has a 99.998% chance of recovery from COVID-19 with no treatment. [Their risk of dying is] 1 in a million. It’s safer than influenza virus. If you gave me a choice, I would rather my kids have COVID-19 than influenza. So, why would I immunize a demographic that has close to 100% chance of recovery with an experimental vaccine that has already killed more kids than the virus?
If you look at the demographic between 18 and 45, people who are healthy have a 99.95% chance of recovery with no treatment … according to the CDC. Same question, why would I vaccinate a demographic that recovers on its own with no treatment?
Third question, if someone has antibodies — and there’s a plethora of evidence [showing] naturally produced antibodies are much more effective in clearing future viruses than vaccine-induced antibodies … Natural immunity is much better, more effective and safer, than vaccine-induced immunity. So, someone who has antibodies already from having COVID before, why would I vaccinate them? …
Fear is an extremely useful tool in manipulating the behavior of people. And that fear has been used to create a psychological motivation to get vaccinated with a vaccine that, in my opinion, has no medical necessity, has tremendous amount of actual and potential risks, and very questionable efficacy.”
Risk Category No. 3 — Long-Term Risks
Beyond the two-to three-year mark are the long-term risks, which are even more difficult to predict. One particularly difficult risk to predict or quantify is infertility. It’ll take decades before we have the data on reproductive effects. Women in their 20s who get the jab might not get serious about trying to get pregnant until they’re in their 30s.
Teens and young children will have to wait decades before fertility can be ascertained. Of course, by then, it’ll be too late. The damage will be done, and hundreds of millions will be in the same boat.
Zelenko cites research published in The New England Journal of Medicine, which concluded COVID vaccination during pregnancy had no increased risk of miscarriage. However, a closer look at the data set revealed that this was only true for women who got vaccinated during their third trimester. Women who get the COVID jab in their first and second trimester have a 24-fold higher risk of miscarriage.
There are also reports of declining sperm counts and testicular swelling in men, and menstrual cycle disruptions in women of all ages. “There is an absolute effect on fertility,” Zelenko says. We just don’t know to what degree yet.
Overall life expectancy is likely to be affected across the board but, again, it’s very difficult to predict just how many years or decades will be lost. Zelenko, like many other doctors, suspect autoimmune diseases and cancer rates will go up as a result of the jabs. As noted by Zelenko:
“Whether you look at the acute spike protein-induced death, the miscarriages, or the myocarditis in young adults, or you look at the subacute pathogenic priming issue, or you look at the potential long-term effects of infertility, auto immune disease and cancer, you have an absolute setup for a genocide. And that’s why these world-leading thought leaders, scientists, are cautioning people …
Let’s do a thought experiment. If COVID-19 were to infect every single human being on this planet and was not to be treated, what would be the overall global death rate? The answer is less than 1%, and I’m not advocating for that, by the way. That’s a lot of people still.
Now, what is going to be the death rate from global vaccination? That is going to be several orders of magnitude greater. And it actually depends how far out you look. Because if someone’s meant to live 80 years and they live 60 years, how do you quantify that? …
We’re talking about 1.5 to 2 billion people [dying] for no reason, except the agendas of a few psychopaths or sociopaths. Why do I say that? It’s because there have been people advocating for population reduction for decades. I just saw a video from [U.K. prime minister] Boris Johnson’s father … advocating for the reduction of England’s population to 15 million …
This type of ideology exists. In this generation, it’s not really anti-Semitic. What it is, is there’s a small group of sociopaths that believe … they’ve evolved into a superhuman enlightened [state] that entitles them the right to dictate the course of history.
For example, Bill Gates in 2015 said the world population needs to be reduced by a certain percentage because of global warming or whatever. So, my question is a very simple question. He’s one of the main supporters and profiteers of global vaccination. Why would I take a vaccine for my health from someone is advocating for the reduction of the world population?
Another scary individual is Klaus Schwab, the founder of the World Economic Forum. He’s very influential. He wrote the book ‘COVID-19 The Great Reset.’ In 2016, in a French interview … Schwab made an announcement that within 10 years, all of humanity will be tagged with an identifier. If you look at the UN 2030 plan, which was crafted by the World Economic Forum, it says ‘America will no longer be a superpower.’
That’s a stated agenda. Then, my favorite is, ‘You’ll own nothing and you’ll be happy. You won’t eat any meat. Fossil fuels will be prohibited. There’ll be a billion refugees, which will have to be integrated into your societies.’ So, my question is, what sociopath feels entitled to make a statement like ‘You will own nothing and you will be happy’?
What entitles this type of individual, or group of individuals, to think that way? Well, they believe that they’re enlightened far beyond the average human or subhuman.”
War Against God
Zelenko, a devout Jew, believes the root of this global takeover is really a war against God. The implication is that life has sanctity, and if life has sanctity, we have human rights, “earned” by our birth alone. This is the source of natural law. And, if we have human rights, handed down by God, then no one has the right to decide how long any one of us should live, or how many people there should be on the planet.
“That’s God’s prerogative,” Zelenko says. “However, if you take that out and view people as no different than an animal, a Darwinist perspective or eugenics perspective, and basically survival of the fittest is the yardstick that you measure the dominance hierarchy of humanity, in that case, these people feel that they are on top of the pyramid, and that entitles them to decide if you and me should live …
I call the [COVID] vaccine ‘Zyklon-V.’ That is the gas the Nazis used to kill my relatives. So to express my sentiments, I call it Zyklon-V. It’s an absolute weapon of mass destruction. People are being lied to, and they’re running into the gas chambers themselves because of the pathogenic fear.”
How to Protect Your Health Post-Jab
If you or someone you know or love got the COVID jab and now have serious regrets, there are definite strategies you can use to protect your health.
It appears if you made it through the first three months OK, then your risk for blood clots is likely radically diminished. To counteract excessive clotting, an anticoagulant may be appropriate. A natural alternative with great promise is n-acetyl cysteine (NAC), as it has both anticoagulant13 and thrombolytic effects,14 meaning it may both prevent clots and break up clots that have already formed. Obviously, do not get any more booster shots.
In the subacute phase, your No. 1 goal will be to avoid ADE. The key to this is to avoid triggering a pathogenic immune reaction, and the only way to do that is to implement some sort of prophylactic protocol, i.e., a COVID, common cold and influenza prevention protocol.
This is especially important for anyone that has received the COVID jab as they are at a high risk of having complications and are under the false impression that they are “protected” when actually they are at increased risk now that they got the jab and need to take extraordinary precautions.
Any symptoms of upper respiratory infection should also be treated immediately, not later. COVID is a multi-phase disease. The first phase is the viral phase, which lasts five to seven days. This is when it’s most easily treated. After Day 7, the disease typically progresses into the inflammatory phase, which requires different treatment.
Zinc supplementation is an important component for prevention and early treatment in the viral stage, as it impairs viral replication. You need to take it with a zinc ionophore, however, such as quercetin, EGCG (green tea extract), hydroxychloroquine or ivermectin.
“The majority of the COVID protocols focus on inhibition of our RNA virus replication. What that means is that for a virus to make copies of itself, it needs to enter the human cell. In the case of RNA viruses, all the COVID, coronaviruses and even the influenza viruses, they use a common pathway called RNA dependent RNA polymerase. That’s a very important enzyme.
That enzyme is what makes copies of the viral genetic material, which then enables for new viruses to be formed and spread. So, if you inhibit the viral RNA replication process, you’ll eliminate viral spreading, viral growth. The beautiful thing about what we found with zinc is that zinc inhibits this enzyme extremely well, if there’s another zinc [molecule] inside the cell.
But zinc cannot really get into the cell on its own. That’s where the concept of zinc ionophores come in. Zinc ionophores opens the door in the cell membrane and allows for zinc to go from outside of the cell, to inside of the cell. And when you increase the concentration of zinc inside the cell, then it can effectively inhibit this enzyme, stopping most if not all, coronaviruses and influenza viruses from replicating.”
If you want to use either hydroxychloroquine or ivermectin and live in a state that restricts their use, look for online telehealth options. The American Frontline Doctors is one resource. They only charge $90 for a consultation and you will be able to get the prescription that you need. Do not use Ivermectin from veterinary sources as it may be contaminated and is not designed for human use.
If you’ve gotten the jab, consider yourself high risk for COVID and implement a daily prophylaxis protocol. This means optimizing your vitamin D, and taking vitamin C, zinc and a zinc ionophore on a daily basis, at least throughout cold and flu season.
In addition to zinc and a zinc ionophore, you also need to optimize your vitamin D level. The range you’re looking for is 60 ng/mL to 80 ng/mL year-round. The appropriate dose of oral vitamin D3 is the dose that gets you within that range.
Vitamin C is another important component, especially if you’re taking quercetin, as they have synergistic effects. To effectively act as a zinc ionophore, the quercetin needs vitamin C.
In an effort to make it easier for patients, Zelenko has developed an oral supplement that contains all four: vitamin C, quercetin, vitamin D3 and zinc. It’s called Z-Stack and can be purchased on zstacklife.com. For a downloadable “cheat sheet” of Zelenko’s protocol for COVID-19, visit VladimirZelenkoMD.com
The take-home message here is that if you’ve gotten the jab, consider yourself high risk for COVID and implement a daily prophylaxis protocol. This means optimizing your vitamin D, and taking vitamin C, zinc and a zinc ionophore on a daily basis, at least throughout cold and flu season.
It would also be useful to do a daily sauna. Ideally one that can heat up to 170 degrees Fahrenheit. The best saunas are far-infrared and have low EMFs. Sadly, I don’t know any that go to 170 degrees and are low EMF.
I use one that goes to 170 and then I turn it off and turn on the SaunaSpace four near IR bulb system in the sauna and go in for 20 minutes. This practice activates heat shock proteins which will help remove the spike proteins and improve other damaged proteins in your body.
If you’re low risk for COVID and have not been vaccinated, make sure you have these items on hand and begin treating at the very first signs of cold or flu symptoms.
Strategies to Lower Risk in Those Who Received COVID Jab
Nebulized hydrogen peroxide 0.1%
Daily or more frequently if needed
NAC (N-acetyl Cysteine)
500 mg once a day
Zinc
15 mg once a day
Vitamin C
500 mg once a day or 250 mg twice a day
Eliminate ALL vegetable (seed) oils
Goal is zero
Vitamin D
Most adults need 8000 IU per day but it is imperative to check blood levels 60-80 ng/ml or 100-150 nmol/l
Daily sauna
20 minutes at 170 degrees will help destroy spike proteins
Time restricted eating
Helps remove spike proteins through autophagy
Seek to eat organic only foods, especially avoid the dirty dozen
This will help limit glyphosate intake
Nebulized Peroxide and Other Health Promoting Measures
In addition to NAC (to prevent and break up clots), vitamin D, vitamin C, quercetin and zinc, buy yourself a tabletop jet nebulizer, some saline solution and food grade hydrogen peroxide. You’ll want to dilute the peroxide with saline to get a 0.1% solution.
Nebulized peroxide is my personal go-to both for prevention and treatment, regardless of the stage the respiratory infection is in. To learn more, download Dr. Thomas Levy’s free e-book, “Rapid Virus Recovery.” As a preventive measure, simply nebulize every other day. Vitamin C is important here too, as it works as a catalyst for the peroxide. A daily dose of 500 milligrams would likely be sufficient for most.
We were forced to remove all the hydrogen peroxide videos that I had previously posted for liability reasons but fortunately they are all now posted on our Substack site. This is important as, in my view, this is the most important step you can take. I would recommend nebulizing a 0.1% solution every day as indicated in the videos, linked below.
There is no danger in doing it every day and likely there is a health benefit. As Dr. Tom Levy describes in one of the videos below, it seems to help improve your bowel movements, which may be a result of eliminating respiratory pathogens that were having negative impact on your microbiome.
Other important health-preserving strategies include the following:
• Make sure you’re metabolically flexible so that your body can seamlessly transition between burning fat and sugar as your primary fuel. This will allow your innate immune system to function optimally. Time-restricted eating is one surefire way to accomplish this.
• Avoid processed seed oils in your diet, such as sunflower oil, corn oil, safflower oil or avocado oils. All contain high levels of linoleic acid, which impairs your mitochondrial function, and in upper respiratory infections, it’s the precursor for the Leukotoxin that occurs in these infections.
• Focus on certified-organic foods to minimize your glyphosate exposure, and include plenty of sulfur-rich foods to keep your mitochondria and lysosomes healthy. Both are important for the clearing of cellular debris, including these spike proteins. You can also boost your sulfate by taking Epsom salt baths.
• To combat the toxicity of the spike protein, you’ll want to optimize autophagy, as this may help digest and remove the spike proteins. Time-restricted eating will upregulate autophagy, while sauna therapy, which upregulates heat shock proteins, will help refold misfolded proteins. They also tag damaged proteins and target them for removal.
It is important that your sauna is hot enough (around 170 degrees Fahrenheit) and does not have high magnetic or electric fields.
• If you’re having post-vaccination symptoms, you could consider:
◦ Low-dose interferons such as Paximune, to stimulate your immune system
◦ Peptide T (an HIV entry inhibitor derived from the HIV envelope protein gp120; it blocks binding and infection of viruses that use the CCR5 receptor to infect cells)
◦ Cannabis, to strengthen Type I interferon pathways, which are part of your first line of defense against pathogens
◦ Dimethylglycine or betaine (trimethylglycine) to enhance methylation, thereby suppressing latent viruses
◦ Silymarin or milk thistle to help cleanse your liver
Of the 700 physicians responding to an internet survey by the Association of American Physicians and Surgeons (AAPS), nearly 60% said they were not “fully vaccinated” against COVID, according to a press release from PR Newswire.
This contradicts an American Medical Association claim — based on 300 respondents — that 96% of practicing physicians are fully vaccinated. Neither survey is representative of all U.S. physicians, but the AAPS survey shows that support among doctors for the COVID injection campaign is far from unanimous.
The AAPS survey also showed that more than half of physician respondents were aware of patients suffering a “significant adverse reaction.” Of the unvaccinated physicians, 80% said “I believe risk of shots exceeds risk of disease,” and 30% said, “I already had COVID.”
“It is wrong to call a person who declines a shot an ‘anti-vaxxer,’ ” AAPS executive director Dr. Jane Orient said. “Virtually no physicians are ‘anti-antibiotics’ or ‘anti-surgery,’ whereas all are opposed to treatments that they think are unnecessary, more likely to harm than to benefit an individual patient, or inadequately tested.”
She went on to say that causality is not proven. “However,” she said, “many of these episodes might have resulted in a huge product liability or malpractice award if they had occurred after a new drug, but purveyors of these COVID products are protected against lawsuits.”
Some info on the censorship by the NZ government and disclosure of the adverse events… from a NZ MD! Deaths, strokes and more. And an alarm sounded about jabbing the children.
“Independent MP Derek Sloan holds a news conference on Parliament Hill to raise concerns about the alleged censorship of doctors and scientists as well as medical information related to vaccines. The Ontario MP has been critical of lockdowns that have been in place due to the COVID-19 pandemic, and also sponsored a petition questioning the safety of COVID-19 vaccines. He is joined by a trio of trio of doctors and scientists.”: https://www.youtube.com/watch?app=desktop&v=vUrp5PlnBwQ&feature=youtu.be&fbclid=IwAR3i7xGctVro2H4AfIbbiqza7Zh0HxCac2jJncDOxLnCCcUemtihE9hzoRQ











![Two more Freudian slips? “[Vaccines] can still kill you even if you’re under the age of 27” – “Millions Have Died From The Vaccines” (The Whitehouse Press Sec. & Sen. Dick Durbin)](https://envirowatchnz.com/wp-content/uploads/2021/07/screenshot-2021-07-20-at-13-59-50-the-markus-allen-show-on-twitter.png?w=672&h=372&crop=1)








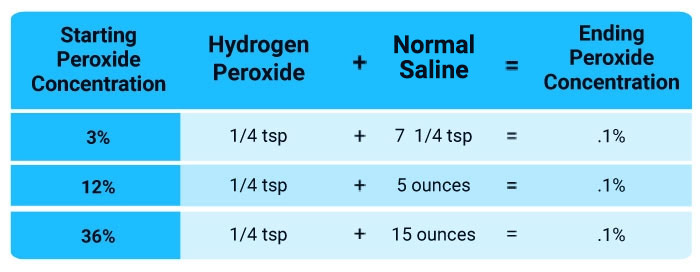





You must be logged in to post a comment.